Article Text

Abstract
Background Teamwork across medical specialties improves patient outcomes. However, it also places an additional strain on team leaders, who must mediate between the medical specialties while at the same time belonging to one of them. We examine whether a cross-training incorporating communication and leadership skills can enhance multispecialty teamwork in Heart Teams and enable Heart Team leaders.
Method In a prospective observational study, the authors surveyed physicians working in multispecialty Heart Teams worldwide, who participated in a cross-training course. Survey responses were collected at the beginning of the course and 6 months later, after course completion. Furthermore, for a subsample of participants, external assessments of course participants’ communication and presentation skills at the beginning and at the end of the training were elicited. The authors conducted mean comparison tests and difference-in-difference analysis.
Results Sixty-four physicians were surveyed. A total of 547 external assessments were collected. The cross-training significantly improved participant-rated teamwork across medical specialties, and communication and presentation skills as rated by participants and external assessors who were blind to the time structure or training context.
Conclusion The study highlights how a cross-training can enable leaders of multispecialty teams in their leadership role by raising awareness of other specialties’ skills and knowledge. Cross-training combined with communication skills training is an effective measure to improve collaboration in Heart Teams.
- assessment
- competencies
- curriculum
- medical leadership
- multi-disciplinary
Data availability statement
Data are available upon reasonable request. Deidentified participant data are available upon reasonable request from the first author.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Some studies show that cross-training improves the performance and effectiveness of multidisciplinary or multispecialty teams, but we do not know why. At the same time, mutual respect of each other’s knowledge and skills is argued to be key for the performance of multidisciplinary or multispecialty teams—but we do not know how to achieve this mutual respect. Finally, we see a growth in leadership and communication trainings for physicians, but we do not know whether these trainings help to develop physicians' leadership and communication skills as perceived by external people who are unaware of the training.
WHAT THIS STUDY ADDS
Our findings highlight a cross-specialty training as a tool to improve respect and appreciation for other specialties’ skills: comparing baseline and post-post training assessments, self-evaluated own skills in other specialties were significantly lower after the cross-training than before. This finding suggests an increased appreciation of other specialties’ skills- and possibly a raised interest in other specialties. Training participants reported an improvement in multispecialty collaboration and conflict resolution at their workplace after the training, reflecting improved teamwork. Finally, we obtained external assessments of leadership and communication skills at baseline and post-post training, which demonstrate the effectiveness of the training in developing physicians into leaders.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Often, career and training paths in medical specialties resemble silos, with specialties keeping mainly to themselves throughout medical school and practice. By showing the value of cross-training for multispecialty collaboration, we encourage joint medical training elements for specialties commonly required to collaborate, and especially those that are considered part of a team, as is the case for Heart Team members or cancer tumour boards. Further, we highlight the need for leadership and communication trainings to be included in medical curricula: our study shows that even for a sample of experienced physicians, a couple of training sessions significantly improved externally assessed communication and leadership skills.
Introduction
Interdisciplinary teamwork in healthcare has been shown to improve patient outcomes.1–5 Focusing on teamwork within the discipline of medicine, providing the best patient care often requires physicians from different medical specialties to combine their distinct skills and knowledge,6–8 thereby collaborating in multispecialty teams. At the same time, different functional backgrounds are a fertile ground for misunderstandings.9 Team members with different medical backgrounds might struggle to communicate with each other due to different jargon and different perspectives.2 10–13 The medical specialty shapes a physician’s professional identity, where physicians from one’s own specialty are the in-group with whom one strongly identifies.14–16 Conflicts might arise in which each specialty defends their own perspective14 15 but lacks understanding of the other specialties’ approaches.17 18 This situation places a particular strain on the team leader, who must mediate between the specialties,11 19 while at the same time belonging to one of them.17 A study20 shows that 22.5% of a sample of Danish physicians shy away from leadership precisely because they want to avoid conflicts with colleagues, and 42.2% would want more training before engaging in leadership.
We evaluate whether a cross-training for (future) leaders of multispecialty teams in healthcare might equip physicians with the needed skills and knowledge that enable them as leaders of such teams. Volpe et al 21 define cross-training as ‘an instructional strategy in which each team member is trained in the duties of his or her teammates’ (p 87). Specifically, cross-training in the form of positional clarification and positional modelling22 might raise awareness and appreciation of other medical specialties’ knowledge and skills. Positional clarification informs about the different subgroups in a team; positional modelling allows team members to observe each other’s task work. By increasing the understanding and knowledge of other specialties, a cross-training might improve multispecialty teamwork23 and facilitate the tasks of the team leader.
We aimed to empirically assess whether a cross-training might improve participants’ communication and leadership skills and multispecialty teamwork. To this end, we examined the effectiveness of a cross-training for cardiac surgeons, interventional cardiologists and other specialists involved in cardiovascular care. The training aimed at fostering the collaboration between medical specialties within ‘Heart Teams’6 and developing participants into Heart Team leaders. Underscoring their practical relevance, Heart Teams are contemplated in practice guidelines.6 Other examples of multispecialty teamwork in healthcare are cancer tumour boards1 and endocarditis teams.7
Answering McGowan et al’s24 call for longitudinal studies which apply rigorous evaluation methods, we aimed at comparing baseline and post-training assessments of skills and confidence, as rated by training participants and external assessors. In this study, we describe the training, analyse variables capturing communication and leadership skills and provide results on the effectiveness of the training with regard to improved teamwork across specialties.
Methods
Study design
This is a prospective observational study. We observe how the analysed training shapes skills, team processes and perceived teamwork for participants who differ ex ante in these skills, perceived teamwork and in medical specialty. We draw on participants and external assessors’ baseline and post-post training evaluations of participants’ skills and teamwork across specialties at participants’ workplaces. First, we surveyed participants at the beginning of the training (baseline measures) and after the training (post-post measures, see ref 25).
Second, we examined how external assessors’ perceptions of participants’ skills and confidence were affected by the training. Professionals in healthcare and communication/psychology evaluated participants’ skills, based on presentations that were jointly prepared by pairs of different specialists on topics in which multispecialty decision-making was involved. The presentations were given in the first and the last training week. The professionals in healthcare and communication/psychology acted as external assessors. They watched 2 min sections of the videotaped presentations that training participants gave in the first and in the last training week. The external assessors did not know that the two presentation segments referred to the beginning and the end of a training course, or that the presentations were given within a training programme. Furthermore, the order in which we presented the presentation segments (first or last training week) was randomised. The use of professionals that were blind to the training setting and the timing of presentations allowed us to estimate a clean training effect.
Study setting
The training was offered by the University of Zurich at the University Hospital Zurich facilities for Heart Team members worldwide. The facilities are fully equipped for live interpersonal interaction, live event transmission, wet laboratories and on-site hands-on simulation using a diversity of low-fidelity and high-fidelity simulators. Our study uses information on three cross-training courses, conducted between October 2018 and April 2020.
Training course structure and contents
The training course consisted of 4 weeks (200 hours) of on-site training and 100 hours of self-study, spread across 6 months. About 60% of the training focused on technical skills, and the remaining 40% referred to communication skills, presentation skills and leadership skills. The trained technical skills consisted of interventional and surgical skills. They were trained via simulations, live cases and case discussions, with worldwide experts in the field as invited speakers and discussion leaders.
Participants were grouped into pairs of different specialists, like one cardiac surgeon and one cardiologist. These pairs jointly presented a clinical case at the end of each of the first three training weeks. At the end of the last week, they presented a jointly prepared thesis. The presentations served the dual purpose of peer teaching and of actively encouraging a collaborative mindset.26 27
To train communication skills, presentation skills and leadership skills, expert trainers gave input and feedback on the structure and content of medical presentations, on how to chair panels around live cases and how to engage in proctoring. They discussed leadership issues, and how to best resolve conflicts in teams.
Due to the 2020 COVID-19 pandemic, the last week of the courses scheduled for the first trimester of 2020 was converted to an online activity.28
Outcome variables
As a first piece of information, we elicited participants’ baseline and post-post ratings of teamwork across medical specialties and disciplines. To capture an overall assessment of teamwork at participants’ workplace, participants rated the items ‘The surgeons and interventional cardiologists here work together as a well-coordinated team’ and ‘The physicians and nurses here work together as a well-coordinated team’ on a 7-point Likert scale29 from ‘Not at all (1)’ to ‘Extremely (7)’. We average over both items (adapted from ref 30, coefficient alpha: 0.60). Note that we capture teamwork across specialties and disciplines from the viewpoint of physicians. The viewpoint of nurses on teamwork with physicians might differ substantially.
To capture knowledge sharing within the team, participants rated the items ‘In the past year, how often has someone at work paid little attention to a statement you made or showed little interest in your opinion?’ and ‘In the past year, how often has someone at work doubted your judgment in a matter of which you had responsibility?’ (ref 31, coefficient alpha: 0.67). Items were rated on a 5-point Likert scale from ‘Never (1)’ to ‘Many times (5)’. We reverse the scale to align higher values with higher knowledge sharing and average over both items. Due to survey length consideration, participants in the 2018/2019 cohort were not given these items to rate in the post-training survey.
To capture the voicing of dissent in the team, participants rated the item ‘It is difficult to speak up if I perceive a problem’30 on a 7-point Likert scale from ‘Not at all (1)’ to ‘Extremely (7)’. We reverse the scale to align higher values with higher speak-up.
Finally, we also capture the resolution of conflicts in the team. Participants rated the item ‘Disagreements are resolved appropriately (ie, what is best for the patient)’30 on a 7-point Likert scale from ‘Not at all (1)’ to ‘Extremely (7)’.
In addition to teamwork measures and in line with the purpose of the training to increase technical skills, communication skills and leadership skills, we elicited participants’ baseline and post-post ratings of their technical skills, and their communication and leadership skills. Regarding technical skills, participants rated their ‘competences in and knowledge of interventional cardiology’, ‘competences in and knowledge of heart surgery’ and part of the sample rated their ‘competences in and knowledge of imaging’ on a 5-point Likert scale from ‘Not at all high (1)’ to ‘Very high (5)’. Regarding communication and leadership skills, course participants rated their ‘communication competences’, ‘presentation skills’, ‘proctoring skills’, ‘competences in running a meeting’ and their ‘confidence as a team leader’ on the same 5-point Likert scale used for technical skills.
As a second piece of information, we had professionals in healthcare and communication/psychology evaluate the skills of the training participants. We restricted this external assessment to skills that might reasonably be evaluated by watching a videotaped presentation. Therefore, we focus on changes in training participants’ confidence (capturing leadership skills32) and their communication and presentation skills. Specifically, we had external assessors rate the item ‘The speaker is confident’ on a 7-point Likert scale from ‘Not at all (1)’ to ‘Extremely (7)’. Regarding communication and presentation skills, external assessors used the same 7-point Likert scale to evaluate how ‘clearly communicated’, ‘to the point’, ‘clear’, ‘memorable’, ‘engaging’ and ‘effective’ the presentation was (items by ref 33).
Statistical analysis
We analysed changes in perceptions of teamwork and team processes, as well as self-rated skills over time, using mean comparisons. Further, we examined differences in skill acquirement between surgeons and non-surgeons using a difference-in-difference approach and clustering SEs on training participant level. Specifically, we regressed participant-rated skills on an indicator variable for the post-post measure versus the baseline, an indicator variable for the participant being a cardiac surgeon and an interaction of the two indicator variables. We controlled for participant gender and age.
As a second piece of information, we compared external assessments of participants’ communication and leadership skills between the first and the last training week using mean comparisons.
Results
Study population
Sixty-four distinct participants enrolled in the different courses, 10 of which participated in more than one course within that time frame. There were 50 male (78%) and 14 (22%) female participants. The average age of participants was 41 years (SD=6.7 years, age range 30–57 years). The participants were established professionals with an average of 9.2 years of experience in their respective fields. They were cardiac surgeons (n=24, 38%), interventional cardiologists (n=36, 56%), non-interventional cardiologists (n=2, 3%), anaesthesiologists (n=1, 2%) and researchers (n=1, 2%).
Sample for the self-assessment of course participants
The population for the first piece of information consisted of the participants in three courses:
First training cohort (2018/2019) with a focus on mitral and tricuspid valve structural interventions, n(baseline)=21 of 24, n (post-post)=12. Eleven participants (46% of the population) responded to both the baseline and the post-post survey.
Second training cohort (2019/2020) with a focus on aortic valve structural interventions, n(baseline)=22 of 26, n(post-post)=25. Twenty-one participants (81% of the population) responded to both the baseline and the post-post survey.
Second training cohort (2019/2020) with a focus on mitral and tricuspid valve structural interventions, n(baseline)=24 of 24, n (post-post)=24. Twenty-four participants (100% of the population) responded to both the baseline and the post-post survey.
Seven participants in the course on aortic valve structural interventions had already attended the first training cohort (2018/2019). Three further participants also attended the second training cohort (2019/2020) with a focus on mitral and tricuspid valve structural interventions. We dropped duplicates to ensure that each participant only featured once (with baseline and post-post responses) in our data set.
In total, we obtained baseline and post-post measures for 53 of the 64 distinct participants in the three courses. The overall response rate for answering at least one survey (baseline or post-post) was 100%, the response rate for answering both the baseline and post-post survey was 83%.
Population for the external blind assessment
The sample for the second piece of information consisted of 547 professionals, of which 262 worked in healthcare and 285 worked in communication/psychology. We recruited the professionals via Prolific (Oxford, UK), which is a company facilitating data collection by providing researchers with panels of participants. The 547 professionals rated 17 training participants, who partook in the first cohort of the training focusing on mitral and tricuspid valve structural interventions, and who consented to having their videotaped presentations rated by such professionals. The average age of the external assessors recruited via Prolific was 30 years, with an average of 8 years of experience. Sixty-six per cent were women.
Training effects on self-rated teamwork
We compare baseline and post-post responses of training participants. Table 1 presents the summary statistics for participant-rated teamwork and team processes, technical skills, communication skills and leadership skills at baseline and post-post the training course. The last column provides the p value of a two-sided t-test comparing the means at baseline and post-post. We find a significant increase in participant-rated teamwork from baseline to post-post the cross-training course. Examining changes in team processes over the course of the training, it seems that participants perceived an improvement in their team’s ability to resolve conflicts but did not register significant changes in knowledge sharing or their ability to voice dissent. Voicing dissent is a vital component of successful teamwork, as otherwise groupthink34 might lead Heart Teams to choose suboptimal treatments.11 35 Thus, we see an improvement in multispecialty collaboration within Heart Teams over the course of the training, which seems mainly due to a better ability to resolve conflicts. Yet, there seems to be room for improvement regarding the voicing of dissent, which seems essential for truly (and not just superficially) resolving conflicts.
Summary statistics: training participant ratings of interdisciplinary teamwork and skills at baseline and post-post
Training effects on self-rated technical skills
The comparison of baseline and post-post measures in table 1 would suggest that the training course did not affect the technical skills of the participants. This is in line with course participants being practising and fully trained physicians. Indeed, the course aim was not to train new skills that participants could incorporate in their clinical practice. Instead, the scope of the clinical training sessions was mainly to cross-educate the students by enabling a positional modelling approach in which cardiologists were training surgeons in their skills, and vice versa. The cross-training activities had the objective to facilitate exchange across medical specialty and cultural barriers. The activities aimed to create a common ground for collaboration, rather than having the objective to reach a competence level to be used in clinical practice. In line with this aim, when analysing specialties separately, we found evidence for an improved appreciation and recognition of other specialties’ technical knowledge and skills.
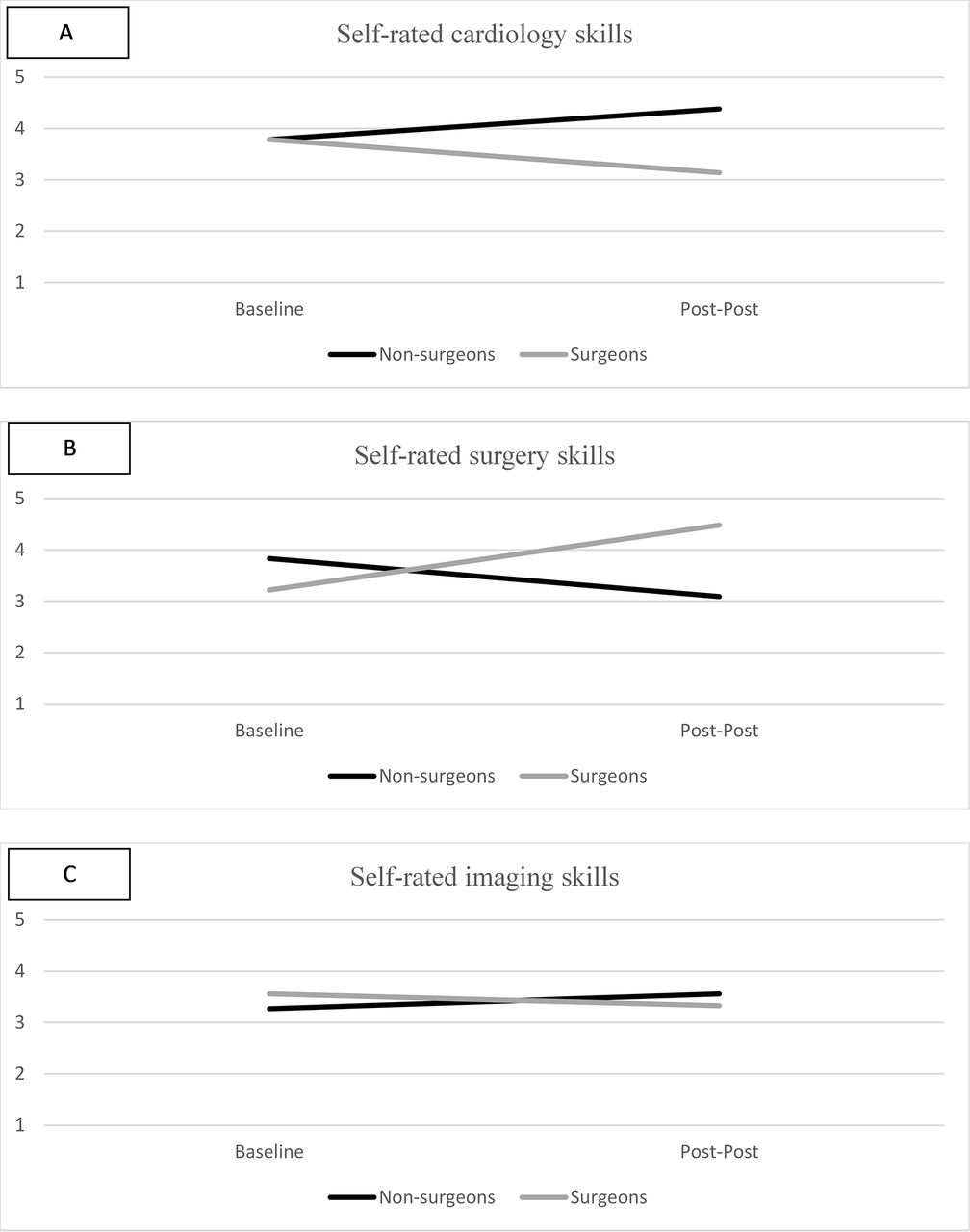
Specifically, we observed a statistically significant difference between non-surgeons and cardiac surgeons in their self-assessment of cardiology and surgery skills: Difference-in-difference analysis revealed that self-ratings of both, surgical skills (p value of interaction between post-post rating and background in surgery <0.001) and cardiology skills (p value of interaction between post-post rating and functional background in surgery <0.001), were affected differently for surgeons and non-surgeons. Figure 1A,B shows that non-surgeons (eg, interventional cardiologists) reported an increase in their cardiology skills and surgeons reported an increase in their surgery skills. This self-rated development of skills is likely due to learning from peers in the same specialty. At the same time, surgeons reported a decrease in their cardiology skills, and non-surgeons reported a decrease in their surgical skills. This decrease in self-rated skills in another medical specialty likely reflects the growing appreciation for the other specialty’s skills, which is the intended effect of positional modelling as part of cross-training. Knowledge and appreciation of other specialties’ skills might also explain the increase in self-reported conflict resolution, because physicians can leverage their knowledge and appreciation of other specialties’ skills to determine the best treatment for the patient.

Self-rated technical skills at baseline and post-post by medical specialty.
Difference-in-difference analysis and figure 1C showed no significant difference in the training-induced development of imaging skills between surgeons and non-surgeons (p value of interaction between post-post rating and background in surgery=0.072). Thus, the training course shaped participant-rated technical skills, but the direction of the change in participant-rated skills depended on the medical specialty and the rated skills.
Training effects on self-rated communication and leadership skills
Communication, the basic process underlying any kind of teamwork, is dependent on team members’ communication skills. Comparison of mean values of baseline and post-post measures revealed a statistically significant increase (see table 1 for p values of two-sided t-tests) in participant-rated communication skills, and their confidence as a leader. We found no change in proctoring skills or skills in organising and managing meetings. Thus, overall, we observed an increase in self-rated communication skills and some aspects of leadership over the course of the training.
Training effects on external blind assessment of communication and leadership skills
Figure 2 presents the box plots for externally assessed communication skills as well as participant confidence in the first (light grey boxes) and the last training week (dark grey boxes). Moreover, we conducted a t-test comparing the within-person means in the first and the last training week. Professionals rated the training participants in the last week compared with the first training week significantly higher in all aspects displayed in figure 2 (p value of two-sided t-test consistently <0.001).

{kind=link}
{kind=link}
Other rated confidence and communication skills in the first (light grey boxes) and the last (dark grey boxes) training week.
Discussion
We found strong support for the training course enhancing participants’ communication skills. Participant-rated communication skills statistically increased from the baseline survey at the beginning of the training course to the post-post survey, which was conducted a couple of weeks after the end of the training course. Furthermore, external assessors’ ratings of participants’ communication skills in the last course week were significantly higher than those in the first training week. In addition to developing physicians’ communication skills, the training course also strengthened their confidence, according to both self-ratings and other ratings. Confidence is often associated with leader status,32 and therefore an important criterion for measuring the training effects on developing physicians into leaders.
A large part of the course content was a cross-training in technical skills, specifically competences in interventional cardiology and cardiac surgery, as well as imaging. At first glance, self-rated technical skills appeared unaffected by the training—when comparing baseline and post-post measures. However, this overall assessment masked interesting differences between non-surgeons and surgeons. When examining these two groups separately, we found that the training increased self-rated skills whenever the participant was already quite proficient in the rated skill, which likely results from learning from other participants.
At the same time, the training seemed to have increased participants’ awareness of their technical skills. Apparently, the non-surgeons realised—by interacting with surgeons—that they knew rather less about cardiac surgery than they had thought. Vice versa, surgeons seem to realise—by interacting with interventional cardiologists and other specialties—how little they knew about interventional cardiology. These insights, although possibly difficult to accept because knowledge is power,35 are an important step towards improved collaboration between non-surgeons and surgeons. Once members of one specialty are aware of how little they know about other specialties’ medical competences, they might be more likely to respect teammates belonging to other specialties and to value their input when discussing treatment options22 (for awareness of different perspectives helping to validate different perspectives9). This respect for other specialties could explain why participants reported improved conflict resolution at their workplace: agreement on the best treatment for a patient is easier to achieve when team members know the strengths and weaknesses of their own approach and that of other medical specialties.36
Supporting a positive effect of the training on collaboration across specialties, course participants rated the collaboration in their Heart Team and their ability to resolve conflicts higher in the post-post survey than at baseline. Thus, the studied cross-training might provide a useful tool in facilitating teamwork in Heart Teams. At the same time, participants perceived no improvement regarding the voicing of dissent. Speaking up and voicing dissent helps avoid groupthink and allows teams to find the best treatment for a patient.11 34 36 Therefore, we encourage further research on how cross-trainings might further encourage psychological safety and trust within a team, so that team members feel safe to speak up and can welcome constructive dissent.36
Limitations
Our study is subject to some limitations. First, the first piece of information relied on a comparison of baseline and post-post self-ratings. Although we would argue that course participants did not remember their answers from the baseline survey when filling out the post-post survey several months later, participants’ answers might be subject to a demand effect, where participants expected that the training was supposed to increase their skills. However, this caveat did not apply to our second piece of information, showing that external assessors rated communication skills higher in the last than in the first training week.
Second, whereas communication skills and confidence can be assessed based on videotaped presentations, we had no such externally evaluated measures for collaboration across specialties or disciplines at participants’ workplaces. Therefore, our analysis relied on participants’ self-ratings. Future research might strive to obtain organisational teamwork measures before and after a training.
Third, the study context of a cross-training for all medical members of Heart Teams allowed us to examine how cross-training might facilitate teamwork across medical specialties. Yet, we did not have access to the non-medical members, such as nurses, pharmacists, dieticians, laboratory scientists or social care representatives. Each of these non-medical members contributes valuable knowledge and skills to the Heart Team, and they might lead the Heart Team at some point during the patient care.36 They might also have different perceptions of interdisciplinary teamwork. Therefore, we call for more research on the effects of cross-training on collaboration between professionals from different disciplines. We expect that a cross-training would enhance familiarity and appreciation of other disciplines’ knowledge and skills. In turn, this would further increase Heart Teams’ effectiveness.36 Nevertheless, such cross-disciplinary trainings might highlight more conflicts and the need to resolve them than cross-specialty trainings: the strong identification with one’s discipline14 15—rather than one’s medical specialty—might create a clearer classification into in-group and out-group, causing conflicts and communication barriers that first need to be resolved before the training might prove beneficial.11 Hence, further research is needed to determine if and if so under what conditions a cross-disciplinary training might improve teamwork in multidisciplinary teams.
Practical implications
Regarding practical implications, our study suggests that to increase collaboration across medical specialties, it is helpful to jointly train physicians from different specialties (similarly, see ref 34). Technical skills should be included in such joint trainings, rather than exclusively training communication and leadership skills. The training of technical skills might help course participants to assess and appreciate the respective skills and competences of other specialties. Cross-training and cross-fertilisation might facilitate collaboration across specialties by helping eliminate barriers between specialties’ cultures.
Considering these findings that showcase the value of cross-training, medical specialties like cardiology and cardiac surgery might need to redraw their training programmes. The aim should be to converge at specific parts of their respective trainings as suggested by Deane and Gournay.17
Conclusions
In many areas of healthcare, putting the patient first might mean putting in place multidisciplinary or multispecialty teams. Rather than hoping for team members to overcome communication barriers and to put aside their competition for resources and prestige, organisations might want to foster collaboration within such teams. Our study indicates training team members’ communication skills combined with a cross-training in technical skills to increase collaboration and to enable team leaders.
Data availability statement
Data are available upon reasonable request. Deidentified participant data are available upon reasonable request from the first author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Human Subjects Committee of the Faculty of Economics, Business Administration and Informatics at the University of Zurich (reference number: OEC IRB 2020-085, approved on 16 November 2020). The project and hypotheses are registered via Open Science Framework at https://osf.io/j46v2. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank Barbara Jenny for excellent support in the evaluation of the training programme. Ramon Gmür and Felix Wüthrich provided exceptional research assistance.
References
Footnotes
Contributors AB set up the paper storyline, planned the study, designed the participant survey and the external evaluation study, conducted the data collection, cleaned and analysed the data, wrote the first draft of the theoretical sections and the results section and contributed to the writing on the other sections. She led the revision process and guarantees the overall content. FM contributed to the storyline and facilitated data collection and results interpretation. He contributed to the writing of the whole manuscript and was involved in the revision process. CAM contributed to the storyline, wrote the first draft of the data and study setting and contributed to the writing of all other sections. He facilitated data collection and results interpretation and contributed to the revision process.
Funding The data collection was partially funded by the Swiss National Science Foundation (grant number: 100018_176358).
Disclaimer The Swiss National Science Foundation was not involved in study design, data collection, analysis or interpretation of data, the writing of the article or the submission decision.
Competing interests AB, FM and CAM were employed at the institution that conducted the evaluated training programme. They do not gain financially or personally from the evaluated training programme. FM discloses grant and/or research institutional support from Abbott, Medtronic, Edwards Lifesciences, Biotronik, Boston Scientific, NVT and Terumo; consulting fees, honoraria personal and institutional support from Abbott, Medtronic, Edwards Lifesciences, Xeltis, Cardiovalve, Occlufit, Simulands and Occlufit; and royalty income/IP rights from Edwards Lifesciences. FM is or has been a shareholder (including share options) of CardioGard, Magenta, SwissVortex, Transseptal Solutions, Occlufit, 4Tech and Perifect. CAM discloses speaker fees from Edwards Clinical Events Committee (CEC) and Cytosorbents.
Provenance and peer review Not commissioned; externally peer reviewed.