Article Text

Abstract
Background The number of female and black, Asian and minor ethnicity (BAME) healthcare professionals has significantly increased over the last few decades. While this highlights the National Health Service (NHS) workforce as diverse and inclusive, most senior managers and conference panellists remain mainly men from Caucasian backgrounds.
Methods We reviewed all publicly available data for major Royal College conferences in the UK from 2015 to 2019 to examine how many of the panellists were men or women and how many were Caucasian or BAME.
Results Our first finding was that publicly available data were available for only 20 out of 70 conferences (29%). At 60% (n=12) of conferences, there were a predominance of male speakers. The median percentage of female speakers remained between 35% and 46%. There were no all-male panels. At 20% (n=4) of conferences in the sample, there were no BAME speakers. The median percentage of BAME speakers remained between 9% and 18%.
Conclusion Conference panels do not yet reflect the diversity of the NHS workforce. We all have a duty to promote inclusivity and diversity in medicine. One way to do this is via conferences, through appropriate actions by conference organisers, panellists and delegates.
- role model
- values
- medical leadership
- engagement
- improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Seventy-seven per cent of UK healthcare workers are women, and almost 50% of UK doctors are women.1 Forty-five per cent of UK doctors and 20% of nurses are from black, Asian and minor ethnicity (BAME) backgrounds.2 3 Over the last decade, every specialty has seen an increase in the proportion of women. Forty-four per cent of National Health Service (NHS) chief executives and 13% of clinical professors are women, but 30% of female managers are BAME compared with 41% of Caucasian women.1
It is important that conference panels reflect this ever-increasing proportion of women and BAME healthcare workers by having a diverse panel of speakers. Previous work examining diversity in other disciplines shows that diversity improves performance, drives innovation and generates better outcomes.4 This would challenge the ‘white male doctor’ stereotype and help reduce unconscious bias that could potentially impact patient care and the doctor–patient relationship.5 The term ‘manel’ describes an all-male conference panel that can mean that academics who are women are not represented. An all-white panel can exclude those who are BAME. Our diverse healthcare workforce needs to be represented at conferences through panels, chairs and delegates, in order to have the greatest impact for our colleagues, patients and future workforce.
The aim of our research was therefore to investigate whether UK Royal College conference panels reflect this increasing proportion of women and BAME doctors.
Methods
We reviewed all publicly available data on conference panels for major UK Royal College conferences from 2015 to 2019 by exploring the Royal College websites to find the annual conference programmes and conducting Google searches on the plenary and keynote speakers and chairs to determine their gender and ethnicity. Data were collected in September 2019.
We investigated conferences of: Royal College of Physicians, Royal College of Surgeons of England, Royal College of Paediatrics and Child Health, Royal College of General Practitioners, Royal College of Anaesthetists, Royal College of Emergency Medicine, Royal College of Psychiatrists, Royal College of Ophthalmologists, Royal College of Pathologists, Public Health England, Royal College of Radiologists, Faculty of Sexual Health, Royal College of Obstetricians and Gynaecologists and The Faculty of Intensive Care.
Results
Our first finding was that data were publicly available for only 20 out of 70 conferences (29%), with no data at all being available for 6 of the 14 Royal Colleges we investigated. Few programmes included information on conference chairs so we could not further investigate the gender and ethnicity of chairs.
However, for the conferences where data were available on keynote speakers, we have divided our findings into the gender and ethnicity categories below.
Gender
At 60% (n=12) of conferences in our sample, there was a predominance of male keynote speakers. From 2015 to 2019, the median percentage of female speakers remained between 35% and 46% (figure 1). In 15% (n=3) of conferences, there were an equal number of male and female keynote speakers. As seen in figure 1, none of the Royal College conferences we examined contained a ‘manel’ and 15% (n=3) of conferences actually had all-female panels.

Proportion of total keynote speakers who were female at Royal College conferences between 2016 to 2019. O&G, RC Obstetrics and Gynaecologists; RCGP, RC General Practice.
Ethnicity
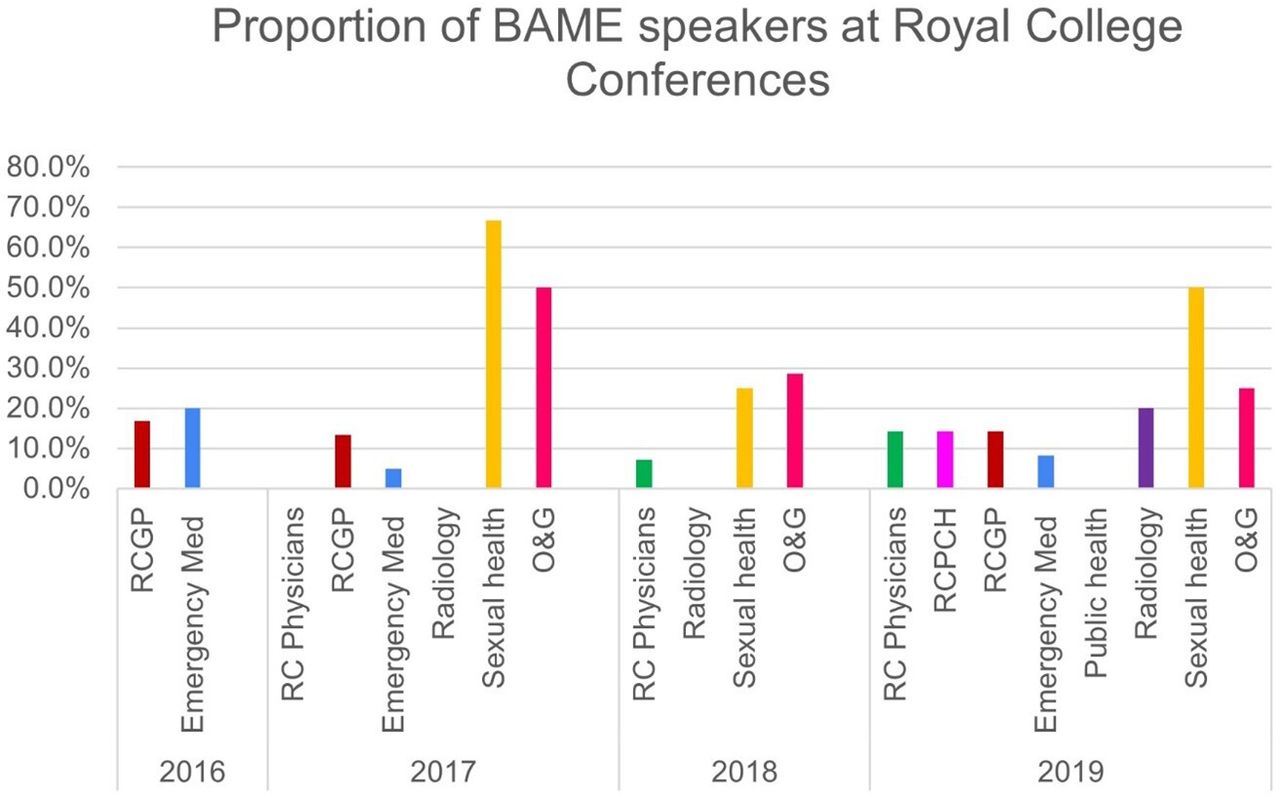
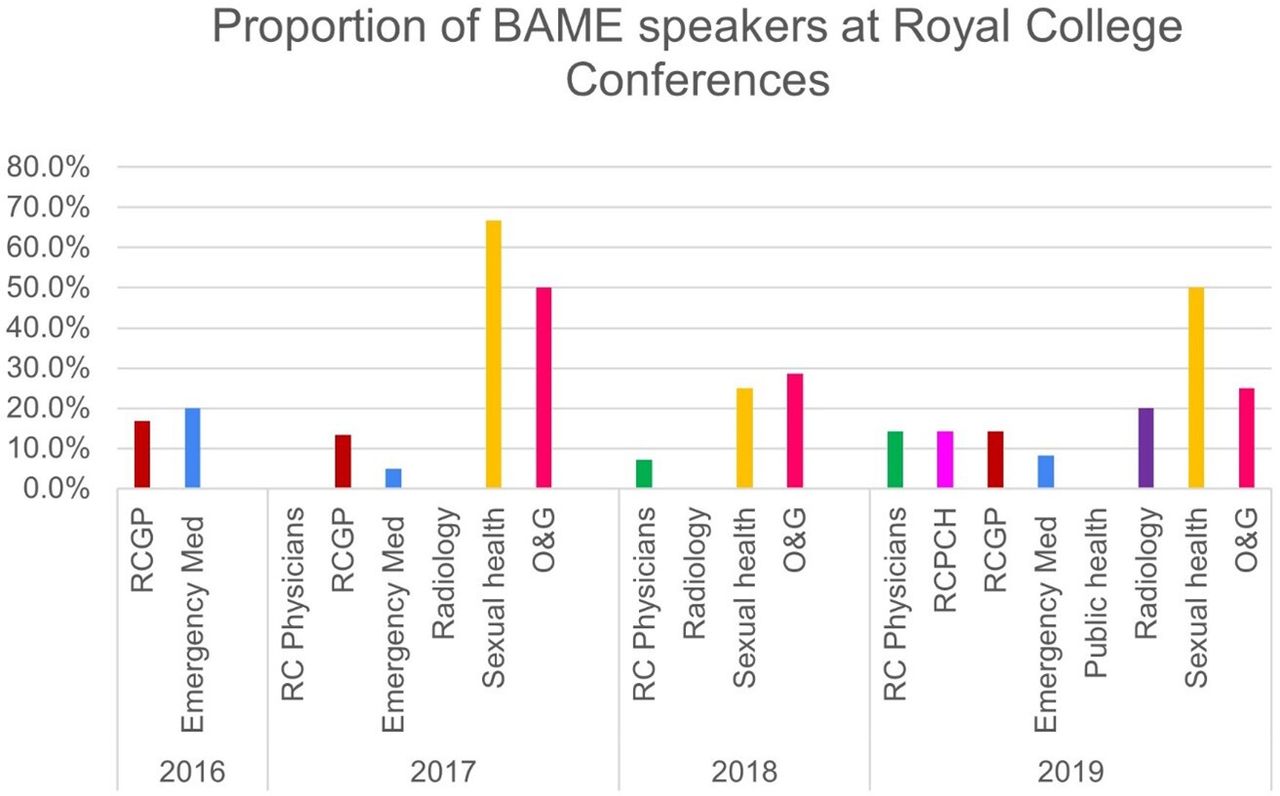
As seen in figure 2, at 20% (n=4) of conferences examined, none of the keynote speakers were BAME. The median percentage of BAME speakers from 2015 to 2019 was between 9% and 18%, but this was not an increase over the 4 years. Only 10% (n=2) of conferences featured an equal number of Caucasian and BAME keynote speakers (the 2019 Faculty of Sexual Health and the 2017 Royal College of Obstetricians and Gynaecologists’ Conference). There was a median of one BAME and nine Caucasian keynote speakers per conference. As seen in figure 2, this was applicable across all specialties.
{kind=link}
{kind=link}
A bar chart showing the proportion of total speakers who were from black and minor ethnicity (BAME) backgrounds at the Royal College conferences from 2016 to 2019. At some conferences, the proportion was 0%, which is why they do not show a bar.
Discussion
Our findings show that the increase in the proportion of women and BAME healthcare workers has not translated into an increased proportion of female and BAME keynote speakers over the last 5 years at Royal College Annual conferences.
One plausible reason for the preponderance of male keynote speakers at conferences is that fewer medical women are in leadership roles and the resulting gender imbalance this imposes. This may be due to the fact that medical women are more likely to have caregiving responsibilities.6 Another review investigating American Royal Colleges has shown this to be a worldwide problem rather than one just existing in the UK.7 The ‘Women Speakers in Healthcare’ group are helping to raise the profile of women speakers and reduce the number of ‘manels’ (all-male panels) at conferences.8 Since the COVID-19 pandemic is reported to have impacted female clinical academics’ careers more than their male colleagues, it is important we continue to address gender equality in clinical academia.9
In terms of ethnicity, there is an even larger disparity between the number of Caucasian and BAME speakers at conferences. The issue of reduced BAME doctors in leadership roles has also been raised in a research report for the General Medical Council that explored how doctors in senior leadership roles establish and maintain a positive patient-centred culture.10 Only one in five of the medical leaders recruited for that study sample were of BAME ethnicity; this is likely due to fewer leadership roles being held by those of BAME ethnicity.10
The recent Black Lives Matter protests have highlighted widespread issues of inequality across the world. In the medical world, healthcare professionals have further realised the importance of addressing this inequality through medical leadership.
Limitations and implications for further work
The main limitation of our study was that only 29% of Royal College conference programmes from 2015 to 2019 were publicly available. This meant that we were unable to identify all of the Royal College keynote speakers from these years. One possible reason for this may have been that many Royal Colleges have a single conference website that is updated each year, so we could only access details for the most recent conference in 2019. The proportion of female and BAME speakers may have differed had we been able to find the data.
We would therefore encourage all the Royal Colleges to keep an archive of their previous conference panel keynote speakers and chairs to enable researchers to scrutinise and examine progress with regard to making Royal College conferences more inclusive.
Another limitation of our research was that we focused on keynote speakers rather than explore poster and oral presentation speakers. Previous studies suggest women are more likely to present posters and men are more likely to have oral and keynote presentations.11
What next
Our work highlights that we need to take further steps to improve diversity of medical Royal College conference panels. This can be addressed at various levels.
Conference organising teams should themselves be diverse, as previous studies show that a gender-balanced team is more likely to organise a gender-diverse panel.11 Resources such as the very helpful ‘Best practice guide’ from the University of Oxford Department of Geography give useful suggestions of improving inclusion at conferences.4 An Elsevier report highlighted that women can struggle to attend international events compared with men,12 and this could perhaps be addressed by allowing speakers to attend virtually, something we have all adapted to doing during the COVID-19 pandemic.
If you are invited to be a speaker at a conference, you can politely ask the organisers how diverse the panel is and highlight the important of diversity of speakers. A Financial Times article highlighted the success of this approach in improving gender diversity in Finance.13 The Lancet has pledged diversity and all editors will only accept invitations to panels if the panel is diverse, and we think this is a very good example that other journals are bound to follow suit.14
If you are a delegate, politely prompt organisers to include a diverse range of panel members to bring this important subject to their attention
While we have primarily focused on gender and ethnicity, it is also equally important to ensure that diversity includes the LGBTQ+ community and those with disabilities.
Concluding remarks
In summary, our research has demonstrated that medical conference panels are not as inclusive or diverse as they need to be. In future, organisers clearly need to be mindful of and prioritise equality in their plenary and keynote speakers. In a similar fashion to The Lancet pledge to diversity, we call on organisations such as the Academy of Medical Royal Colleges, Association of American Royal Colleges, Academy of Medical Sciences and Royal Society of Medicine to also pledge for diversity and inclusion. Events such as the recent NIHR Academy 2020 Conference on inclusivity and diversity help raise awareness. The American Economic Association includes diversity in conferences as part of their Best practices for Economists15 and perhaps the General Medical Council could do the same for doctors.
Each of us have the duty and power to bring about more inclusivity in clinical academia. Only by achieving inclusion and diversity throughout clinical academia will we all benefit and contribute to achieving the equality related Sustainable Development Goals.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Professor Henrietta Bowden-Jones and Dr Katherine Sleeman for encouraging us to write up and submit this work for publication. Thank you to the University of Manchester for providing funding for our paper to be published open access.
Footnotes
Contributors NPB conceptualised the paper. Both authors undertook data collection, analysis, literature review, writing and finalising the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.