Article Text

Abstract
Background Male hospital consultants earn 13% more than their female counterparts. The intersectional effects of ethnicity and gender are not known.
Objective To describe and analyse the mean bonus pay gap in terms of gender and ethnicity for consultants across the Shelford Group.
Design Cross-sectional study.
Setting Hospitals in the Shelford Group.
Participants Shelford Group hospitals.
Main outcome measures Mean bonus pay gap for male vs female and White vs Black, Asian, Minority Ethnic (BAME) consultants.
Results Seven of the 10 Shelford Group hospitals provided data for financial year 2018/2019. The average mean bonus gender pay gap was in favour of male consultants (30%; range 12%–48%), and also favoured White consultants compared with BAME consultants (17%; range 7%–31%). The average mean bonus pay gap between White male and BAME male consultants was 20% (range 7%–34%) in favour of White male consultants, while that for White male and BAME female consultants was 46% (range 26%–60%) in favour of White male consultants.
Conclusions Our data show for the first time that there may be an intersectional effect of gender and ethnicity associated with mean bonus pay for consultants. Action is needed to address this imbalance.
- consultant
- clinical leadership
- medical leadership
- reward
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The proportion of NHS doctors who are female has grown every year since 2009. Thirty-seven per cent of consultant roles are now held by female consultants compared with 30% in 2009.1 The proportion of consultants from Black Asian and Minority Ethnic (BAME) groups is around 38% and growing.1 The Department of Health and Social Care recently released Mend the Gap: The Independent Review into the Gender Pay Gap in Medicine.2 This report highlighted that male hospital consultants earn 13% more than their female counterparts, even when part-time working is accounted for. Clinical Excellence Awards (CEAs) form the large majority of bonus pay for consultants and are part of a competitive renumeration system. They recognise and reward NHS consultants who perform ‘over and above’ the standard expected for their role and aim to reward the consultants who contribute most to the delivery of safe and high-quality care and the improvement of NHS services.3 They are not awarded automatically and must be applied for through local and national committees.
A significant amount of research has been conducted on the superimposing or intersectional effects of gender and ethnicity outside of medicine.4 Organisations have been shown to play a key role in generating and perpetuating inequality in bonus pay outcomes.4 There is a paucity of information and research on the intersectional effects and associations of gender and ethnicity within NHS leadership.
We analysed gender and ethnicity bonus pay gap data for consultants working across the Shelford Group of hospitals to begin to understand if there are intersectional associations of gender and ethnicity on bonus pay awarded.
Methods
Freedom of Information requests were sent to the 10 Shelford Hospitals. The Shelford Group is a collaboration between 10 of the largest teaching and research NHS hospital trusts in England. Together they account for over £12.5 billion of the NHS budget, care for around 17 million patients a year, employ over 140 000 staff (11% of the NHS workforce)1 and account for two thirds of the country’s clinical research infrastructure.5 Collectively, its members are ‘strategically significant to the NHS nationally and are dedicated to excellence’. Equality and Diversity are highlighted as a priority in their policy.5 The first Freedom of Information request was sent 01/2020 with two reminders sent every 3 months if no response, with maximum of two reminders. Data were requested on the mean bonus pay gap for male vs female consultants, White versus BAME consultants and White male versus BAME female consultants for the financial year 2018/2019. Where mean bonus pay data was provided, the mean bonus pay gap was calculated using standard government guidance.6 Data were analysed using simple descriptives.
Patient and public involvement (PPI)
We did not involve patients and the public in this study. Findings will be disseminated through appropriate networks including the British Medical Association and Medical Women’s Federation.
Results
Of the 10 Shelford Hospitals, seven provided data for 2018/2019. No data were provided by Imperial College and Sheffield Teaching Hospitals NHS Trusts, while Newcastle Upon Tyne Hospitals only provided 2017/2018 data. Two NHS Trusts (Manchester University Foundation Trust and University College London Hospitals Foundation Trust) reported that they do not routinely collect data for ethnicity and therefore only provided data related to gender.
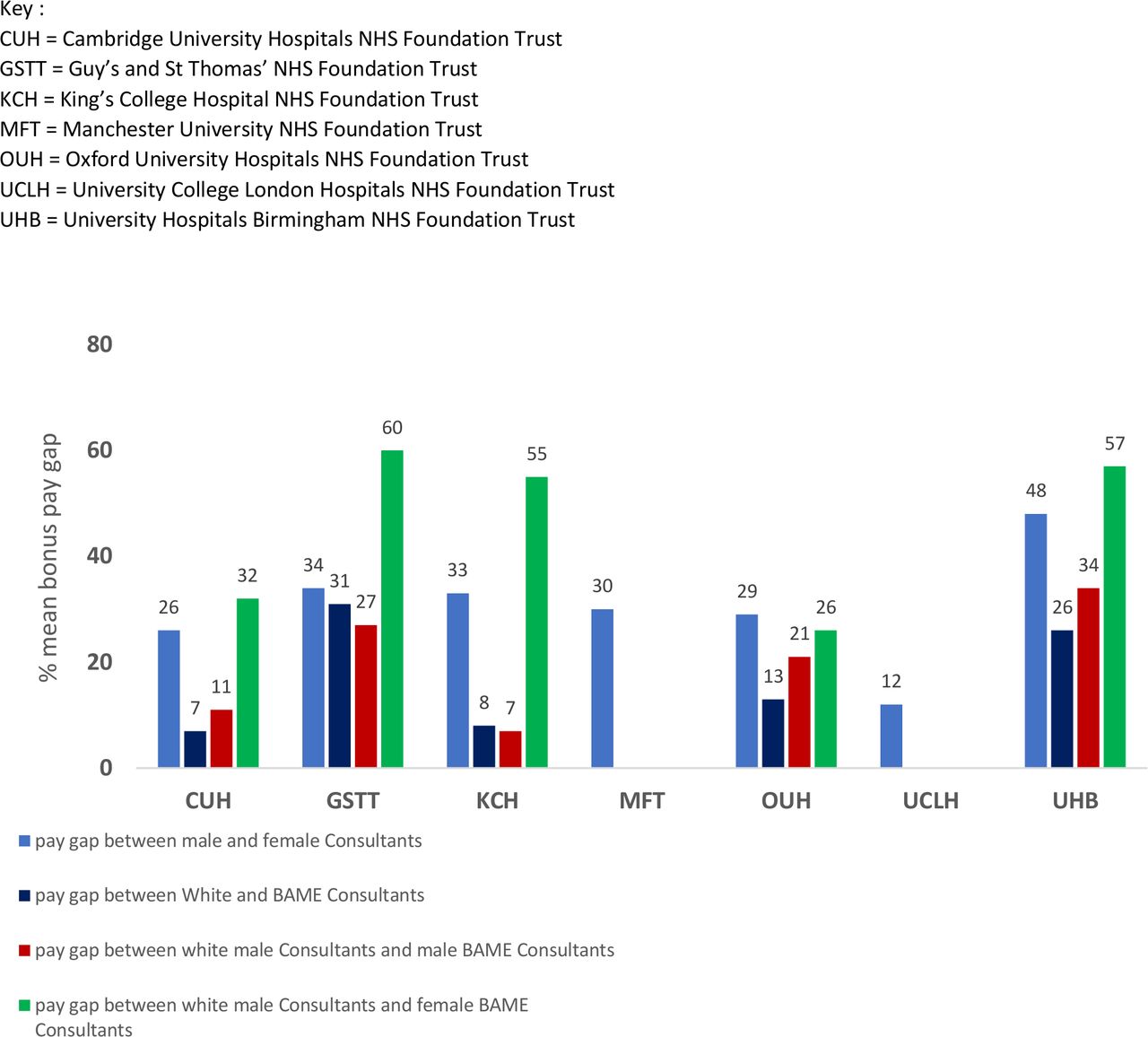
The average mean bonus pay gap for male and female consultants was 30% (range 12%–48%) in favour of male consultants. The average mean bonus pay gap for White and BAME consultants was 17% (range 7%–31%) in favour of White consultants. The average mean bonus pay gap between White male and BAME male consultants was 20% (range 7%–34%) in favour of White male consultants. The average mean bonus pay gap between White male and BAME female consultants was 46% (range 26%–60%) in favour of White male consultants (figure 1).
{kind=link}
Percentage mean bonus pay gap for Shelford Hospital consultants financial year 2018/2019 analysed by gender and ethnicity. BAME, Black Asian Minority Ethnic.
Discussion
We aimed to analyse bonus pay gap data to begin to understand if there are intersectional associations of gender and ethnicity on bonus pay awarded. Our results indicate that there was a mean bonus pay gap associated with both gender and ethnicity for consultants in the Shelford Hospitals for the financial year 2018/19.
These data agree with national data showing a significant mean bonus pay gap associated with gender in favour of male consultants. However, we are the first to analyse and show that there is also a bonus pay gap associated with ethnicity in favour of White consultants. Importantly, our data show a superimposing or intersectional association with gender and ethnicity, with female BAME consultants within the Shelford Group receiving the lowest bonus pay for all consultant groups examined. Whether the large mean bonus pay gap demonstrated, represents gender and ethnicity bias, or self-selection is not clear. However, reflection on these data considering the recent findings from the Commission on Race and Ethnic Disparities report7 on the lack of institutional or structural racism within the UK, is important.
Of note, national data suggest that female consultants are under-represented in applications for national CEA awards but have an approximate equivalent chance of success when they do apply.8 BAME consultants are both under-represented in application rates and less likely to receive awards when they do apply.8 It is possible that a competitive renumeration system underpinned by self-advocacy, favours White consultants. Unfortunately, there are no national data available on the application and success rates of those who are both female and BAME. Decision making committees nationally continue to be under-represented for those from BAME groups.
Limitations
We were limited by incomplete return of data from two hospitals and no return of data from a further two hospitals. One hospital did not provide data for 2018/2019. Shelford hospitals may not be truly representative of all hospitals in England but do represent a significant proportion of the NHS consultant workforce. The average mean bonus pay gap calculation did not take account of the variable staff numbers in each group and across services. In addition, it did not take account of career stage. We could not test whether the differences observed were statistically significant as most hospitals provided only the mean bonus pay gap between the groups examined.
We recommend routine collection and transparent reporting of intersectional gender and ethnicity data for bonus consultant pay both locally and nationally. It is possible that even explicit acknowledgement of differences may itself act as an intervention to redress imbalance. Trusts should actively support BAME and female consultants in their applications and ensure that decision making committees reflect the diversity of consultants within the NHS.
Conclusion
There may be a superimposing intersectional effect of gender and ethnicity associated with the awarding of CEAs to consultants working within the Shelford Hospitals. Further investigation on reasons for this, and whether this is a widespread issue within the NHS is urgently needed.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
Esther Jewson for advice on wording of the Freedom of Information Request and Bella Millett for administrative assistance.
Footnotes
Twitter @SBajwah
Contributors SB designed the study. AO conducted the data analysis. SB drafted the manuscript. SB and AO critically revised the manuscript for important intellectual content. Both authors approved the final version of the manuscript. SB is guarantor. The corresponding author attests that all the listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was conducted on behalf of the Cicely Saunders Equality, Diversity and Inclusion Committee.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare; no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. SB and AO report grants from the Medical Research Council [MR/V012908/1], National Institute for Health Research (NIHR) Applied Research Collaboration, South London, and Cicely Saunders International outside the submitted work. SB self identifies as a female British Pakistani and works clinically at both King’s College Foundation Trust and Guys and St Thomas NHS Foundation Trust; AO identifies as a female from BAME background.
Provenance and peer review Not commissioned; externally peer reviewed.