Article Text

Abstract
The National Health Service in England has largely relied on a human resources trilogy of policies, procedures and training to improve organisational culture. Evidence from four interventions using this paradigm—disciplinary action, bullying, whistleblowing and recruitment and career progression—confirms research findings that this approach, in isolation, was never likely to be effective. An alternative methodology is proposed, elements of which are beginning to be adopted, which is more likely to be effective.
- effectiveness
- Recruitment
- management
- strategy
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Staff are healthcare’s biggest cost and greatest asset. How staff are treated impacts significantly on their health and well-being, on organisational effectiveness and on the care patients receive. Despite (and arguably sometimes because of) the efforts of human resources (HR) and organisational development specialists, staff experience in the National Health Service (NHS) falls well short of strategic aspirations.
The problem
Organisational cultures influence workforce health and well-being, organisational effectiveness and safe, effective patient care. Scrutiny of four particular NHS employment practices proposed as improving organisational culture suggests the dominant HR paradigm of recent years is flawed. Each of these four practices, addressing bullying and harassment; enabling and protecting staff raising concerns; ensuring disciplinary action is fair and appropriate; and preventing discriminatory recruitment and career progression, is considered in turn. They are chosen because all four share a common methodology, provide accessible large-scale NHS data, are significant in influencing workplace culture, are prone to bias, and each impacts on workforce experience, organisational effectiveness and patient care.
The role of HR
The most recent NHS People Plan1 adopts a unitarist assumption that everyone benefits from effective management, framing the workforce as a strategic asset, highlighting correlations between workforce treatment and better outcomes for staff, employers and patients.
Seeking a strategic role, NHS HR has delegated much operational responsibility to line management, but workload pressure and organisational turmoil mean line managers’ management capacity and skills often fall short of delivering their devolved HR responsibilities often leaving HR teams struggling to translate HR intentions into desired outcomes.
Evidence for the impact of HR interventions on staff well-being and treatment, organisational effectiveness, and patient experience and outcomes is mixed. There is evidence of strong links between certain management practices (well-structured appraisals, good team working) and patient outcomes2 but others question how strong the wider evidence is.3
Methodological individualism
Every NHS organisation has policies, procedures and training claiming to set fair, equitable standards which enable individual staff to raise concerns, confident they will be heard fairly and will suffer no resultant detriment. This HR paradigm has, until recently, dominated much NHS employment practice including on ‘speaking up’, bullying, disciplinary action, and on recruitment and career progression, but with little evidence of success.
On bullying, for example, Evesson et al4 concluded
‘while policies and training are doubtless essential components of effective strategies for addressing bullying in the workplace …… research has generated no evidence that, in isolation, this approach can work to reduce the overall incidence of bullying in Britain’s workplaces.’
Training is the default approach to mitigating bias in all four interventions, but while diversity training may improve cognitive understanding and beliefs, its effects fade over time5 while unconscious bias training (popular in the NHS) may assist those who wish to learn, but its impact on decision-making is limited or unproven.6
Bullying
One-quarter of NHS staff, notably disabled, lesbian, gay, bisexual, and transgender (LGBT)+ and black and minority ethnic (BME) staff, report bullying by managers or colleagues7 damaging staff health, organisational effectiveness and patient care. Bullied staff are less likely to admit mistakes, raise concerns or work in effective teams as the trust, collaboration and communication essential for good care are undermined by bullying and incivility. Bullying and discrimination increase turnover, absenteeism and presenteeism for both witnesses and victims, with substantial financial costs to employers.8
NHS Employers bullying guidance (2006–2016) stated ‘employers can only address cases of bullying and harassment that are brought to their attention.’9 Yet much research repeatedly concludes many bullied staff stay silent, believing nothing will change or that reporting might make things worse. Reliance on policies and procedures for dealing with bullying,
‘flies in the face of current research evidence about the limited effectiveness of using such individualised processes to resolve allegations of bullying and to prevent bullying behaviours.’10
Many grievance, discipline and whistleblowing procedures risk a punitive, expensive and adversarial approach, likely driven by risk mitigation with an eye on possible litigation11 while pressures on HR practitioners undermine effective conflict resolution which in turn ‘could encourage an emphasis on procedural and legal compliance as opposed to a focus on the promotion of positive relationships inside the workplace.’12
Whistleblowing
NHS policy stresses staff must be free to raise concerns without fear of detriment, but numerous NHS scandals and many more incidents are characterised by a failure to do so. Francis13 found that reliance on individuals raising concerns when staff might fear adverse career and health consequences was ineffective, noting BME staff were less likely to be listened to and more likely to be victimised when speaking up. NHS staff survey data reports just 62.0% of NHS staff feel safe to speak up about concerns overall in their organisation (though higher for clinical concerns) and many lacked confidence their employer would address their concern. Interestingly, more NHS staff were willing to speak up on clinical concerns—possibly because staff feel a greater obligation to flag clinical issues (and feel able to do so without being seen as troublesome). The Freedom To Speak Up Guardian system Francis recommended relies primarily on individuals raising concerns and is largely dependent on variably supportive local organisational climates.14
Discipline
All NHS employers have disciplinary policies, procedures and training intended to set standards, which (in theory) emphasise learning but in practice may prompt blame, prolong processes, be adversarial and, like referrals to professional regulators, be prone to bias against BME staff. But it took a nurse suicide arising from such failures for NHS leaders to acknowledge the current paradigm has serious shortcomings.15 16
Recruitment and career progression
Recruitment and career progression is prone to bias which influences person specifications, advertising, shortlisting, appointment from shortlisting, appraisals, feedback, access to ‘stretch opportunities’ and onboarding. For example, it remains 1.54 times more likely that a white NHS shortlisted candidate will be appointed compared with a shortlisted BME candidate.17
One large scale analysis of interventions to improve diversity in recruitment and career progression found policies and procedures were underpinned by ‘methodological individualism’ and were ineffective or counter-productive without accountability, while
‘practices that target managerial bias through feedback (diversity evaluations) and education (diversity training) show virtually no effect in the aggregate… five years after instituting training for managers, companies saw no improvement in the proportion of white women, black men, and Hispanics in management, and the share of black women actually decreased by 9%, on average’.18
A review of HR staff experience in the NHS in London found that despite a raft of policies, procedures and training there was ‘a lack of BAME representation across the most senior roles in organisations… concerns were raised with regard to the unfairness of HR practices such as recruitment and secondment policies and procedures.’19
What might an alternative paradigm look like?
Organisational culture is shaped by formal organisational values and local policies; by values, behaviours and knowledge that staff learn; and by how an organisation’s leaders behave. Culture is crucial in healthcare. Managing staff with respect and compassion correlates with improved patient satisfaction, infection and mortality rates, Care Quality Commission ratings and financial performance.20
An inclusive climate is more likely to enable psychological safety and both are likely to positively influence speaking up, and may be particularly helpful in the hierarchical environments common in healthcare (where it may minimise the effect of status on psychological safety within teams and give legitimacy to voice.21 22 Where diversity is underpinned by inclusion, research suggests staff well-being, organisational effectiveness (turnover, innovation, engagement, team working) and patient care and safety are likely to improve.
Drawing on accountability theory and research on mitigating bias, we may, therefore, construct an alternative HR paradigm more likely to positively contribute to organisational cultures supporting inclusion, psychological safety, staff well-being, organisational effectiveness and patient care.
Theme 1: accountability
Individuals required to justify their decisions to more senior people are likely to undertake more thoughtful evaluations. When decision-makers were required to explain their responses to a partner, women were less likely to be held to a higher standard of competence than men.23 The awareness of accountability acts to pre‐empt the introduction of bias into hiring decisions before it happens and challenges stereotypes when making decisions.24 Thus, inserting transparency (publishing each unit’s average performance rating and pay raise by race and gender) prompted accountability and almost eliminated an ethnicity pay gap.25 Applying this more generally (e.g, to closing the gender pay gap) would require debiasing discriminatory work practices and inserting accountability.
Goals motivate through inserting accountability as an expectation that individuals (or the organisation) might be required to justify their acts or omissions to others.26 Setting goals resulted in markedly higher performance than not doing so.27 When specific (senior) staff or entities (such as a diversity task force) were tasked with accomplishing diversity goals those goals were more likely to be achieved.28
Theme 2: leadership
Whether organisational and team leaderships are inclusive and promote psychological safety greatly influences whether strategies on whistleblowing, bullying, disciplinary action, and recruitment and career progression, are effective and sustainable.
Inclusive leadership is needed to manage the psychological responses of individuals that result from social categorisation processes29 and can enable effective team working in diverse teams. Support from top management is a key factor in determining the success of diversity programmes.30 In contrast where diversity interventions lack the involvement of top managers and fail to address overall work processes, their long-term effectiveness in transforming organisational culture is likely to be limited.31
What leaders focus on, talk about, pay attention to, reward and seek to influence, tells staff what leadership values they should take note of.32 Staff networks can play a significant role in ‘holding feet to the fire’ and illuminating lived experience but to what effect may well depend on whether leaders recognise their value.
Theme 3: debiasing processes not just people
Both conscious and unconscious biases are ubiquitous and powerful. They are frequently institutionalised through policies and practices that systematically advantage some groups and discriminate against others. Over-riding stereotypes requires conscious decision-making, whereas activating stereotypes can occur automatically. Stereotypes impact the behaviours and judgements of individuals regardless of their own protected characteristic. Research suggests mitigation of bias requires a focus on mitigating bias in systems and processes rather than a reliance on removing it from individuals as illustrated below.
Employment relations issues (bullying and discipline)
Using formal grievance procedures to tackle bullying is rarely effective. Individual employees who ‘win’ often find they have to ‘move on’ while employees find underlying causes are rarely addressed. Staff who do raise bullying concerns generally want bad behaviours to stop rather than to lodge formal grievances; many NHS organisations recording few formal complaints report high levels of bullying in anonymised surveys.
Disciplinary action (which in the NHS may overlap with referrals to professional regulators) is nominally focused on learning but in practice has frequently emphasised blame. Of the four HR interventions considered, it is the only one that appears to have seen improvement in the last few years. The number of NHS cases fell by 36% in 2018–2021 while the gap between the relative likelihood of white and BME staff being disciplined radically reduced 2016–2021.33
While no single causal effect has been identified for this improvement, evidence from multiple Trusts suggests two specific interventions emphasising accountability and learning may have been effective. First, large numbers of employers now insert an accountability nudge (or bias interrupter) at the ‘point of incident’ requiring line managers considering launching an investigation to pause and explain to a senior manager why a formal investigation rather than an informal discussion is appropriate, often linked to awareness of risk of racial bias. Second, a increasingly adopted ‘just culture’ initiative in Mersey Care NHS FT emphasising early informal intervention alongside learning not blame has incentivised a learning culture, replacing a retributive culture with a restorative one, also leading to substantial financial savings.34
The NHS has shown growing interest in early, informal, proactive, systemic bullying and incivility interventions—a ‘public health’ approach such as the ‘professionalism pyramid’ developed by Vanderbilt University’s Center for Professionalism and Patient Advocacy, which emphasises discussing unprofessional behaviour at the first signs of it and providing support for the individual to change while emphasising the need for interventions to escalate if unprofessional behaviour persists or worsens. A review found the majority of professionals involved ‘self-regulate’.35 The drivers of workplace bullying and incivility are stronger when demand outstrips staff capacity (as they do currently). The evidence base for management or bystander training on bullying, however, is not yet convincing.
Whistleblowing
Wu et al36 argue that while improving clarity, fairness and quality and transparency of policy, process and procedure may be a prerequisite, clarity and consistency of procedure can only go so far, and indeed the addition of further layers of formal policy may provide a veneer of order without enhancing understanding.
Nembhard37 suggests individuals located lower in formal hierarchies tend to routinely yield to higher-ranking employees in social situations. Reitz and Higgins38 similarly highlight the ‘power imbalance in organisational roles (as) perhaps the most important factor that makes employee silence such a common experience’ and go on to argue that leaders should focus ‘their attention and efforts predominantly on those who feel silenced, urging them to ‘be brave’, ‘speak up’ and have the ‘courageous conversations’ that are required…… We need to stop trying to ‘fix the silenced’ and rather ‘fix the system’. Crucially, Reitz and Higgins conclude ‘instigating whistleblowing lines and training employees to be braver or insisting that they speak up out of duty, will achieve little therefore, without leaders owning their status and hierarchy, stepping out of their internal monologue and engaging with the reality of others’.
Accountability and inclusive leadership (and psychological safety), not policies, procedures and training in isolation, are crucial in creating an open, safe culture.
Recruitment and career progression
Kalev et al found39:
Structures that embed accountability, authority and expertise (affirmative action plans, diversity committees and task forces, diversity managers and departments) were the most effective means of increasing the proportions of white women, black women and black men in private sector management.
Responsibility structures make training, performance evaluations, networking and mentoring programmes more effective.
Ovseiko et al40 found the decision by the UK National Institute for Health Research not to shortlist NHS organisations or university partnerships for grants unless their academic department held at least a silver Athena Swan award (recognising policies to promote sex equality) prompted large increases in women in leadership roles.
Research suggests a number of ways in which debiasing of recruitment and career progression may be effective. Bohnet41 draws on randomised controlled trials which to identify a range of evidence-based interventions that can mitigate gender bias such as joint evaluation. Google developed an approach to interrupt recruitment bias emphasising a clear and detailed job description; structured behavioural interviews in which information was collected independently on a range of data points such as work samples; and rigorously structured interviews, with a final decision made by a hiring panel which need not include the future line manager.42 43
Bias interrupters are likely to be much more effective than a reliance on diversity training. Numerous interventions are likely to both mitigate bias throughout recruitment and career progression and to select better candidates.44
Conclusion
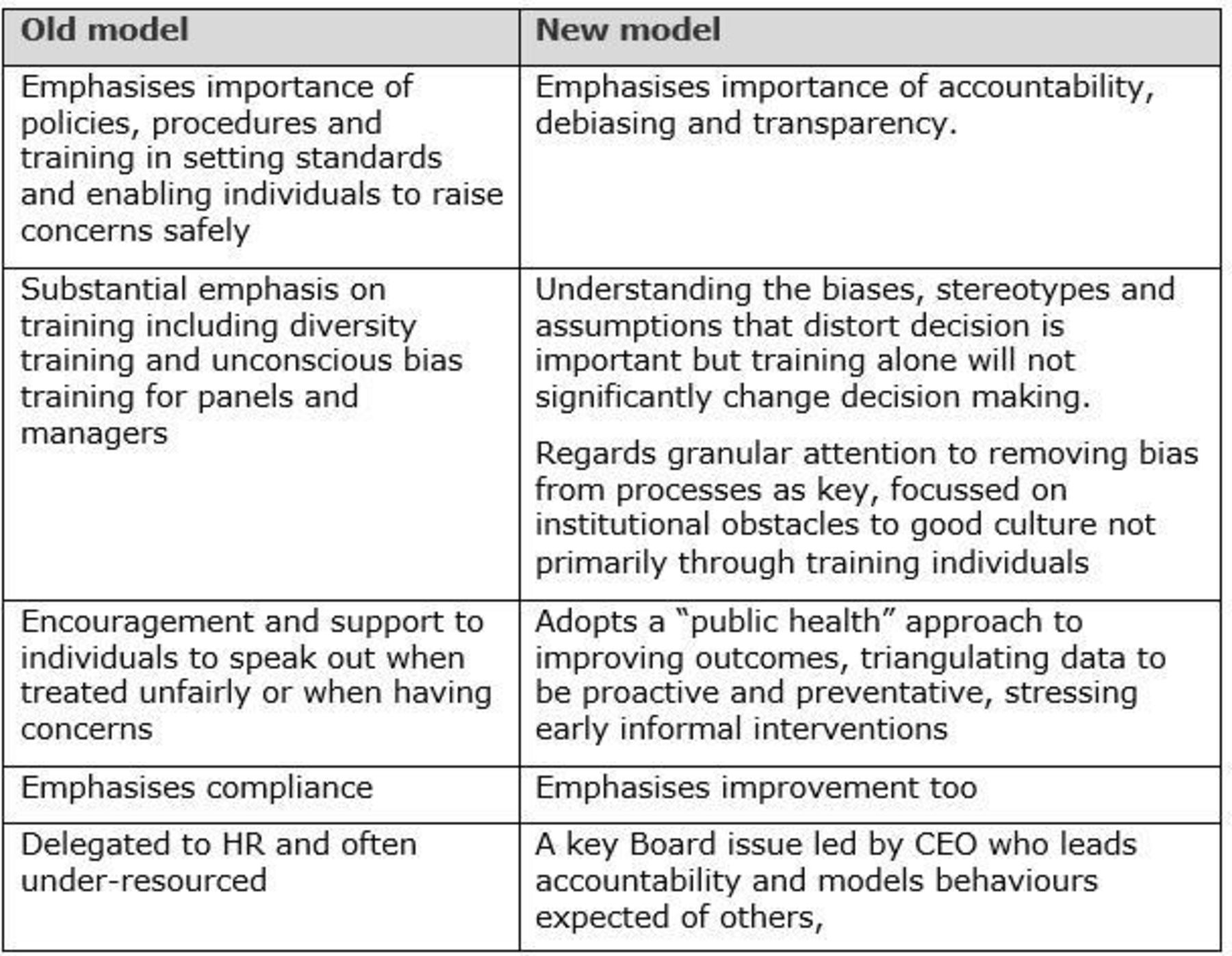
Figure 1 summarises the contrast between the old and new HR paradigms:
{kind=link}
Schematic: the old and the new HR paradigms. CEO, chief executive officer; HR, human resource.
Applying this alternative HR paradigm requires a balance between motivation and mandation—a theory of change which understands that ‘a particular behaviour will occur only when the person concerned has the capability and opportunity to engage in the behaviour and is more motivated to enact that behaviour than any other behaviour’.45 In the NHS, an effective theory of change will require a narrative emphasising improvement as well as compliance, and an approach that recognises the need to change staff behaviours alongside board-led interventions.46 The narrative will need to emphasise the importance of inclusion linked to psychologically safe teams if improvements in these four metrics are to be sustainable.
A primary reliance on policies, procedures and training will not, in isolation, reduce bullying, improve the effectiveness or safety of whistleblowing, create a disciplinary environment focused on learning, or recruitment and career progression underpinned by fairness.
An alternative approach, rooted in accountability theory and an understanding of how to mitigate bias, is significantly more likely to both improve these indicators and help create a culture of inclusion and psychological safety that evidence suggests is effective and appropriate in healthcare. The proposed methodology is much more likely to signpost interventions leading to intended outcomes.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @rogerkline
Contributors RK is the sole author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.