Article Text

Abstract
Background Healthcare organisations are increasingly placing the onus on care providers to lead change initiatives to improve patient care. This requires care providers to perform tasks in addition to their core job roles and often outside of their formal training. The existing literature provides few insights regarding the functions required of change leaders in healthcare organisations.
Objective To identify the core functions required of effective change leaders in healthcare organisations.
Design Qualitative interview study.
Participants Data were collected from semistructured interviews with 31 individuals employed by a large cancer centre in a variety of different positions (eg, surgeons, anaesthesiologists, nurse anaesthetists, nurses, project consultants and research coordinators) who had been involved in successful quality improvement initiatives.
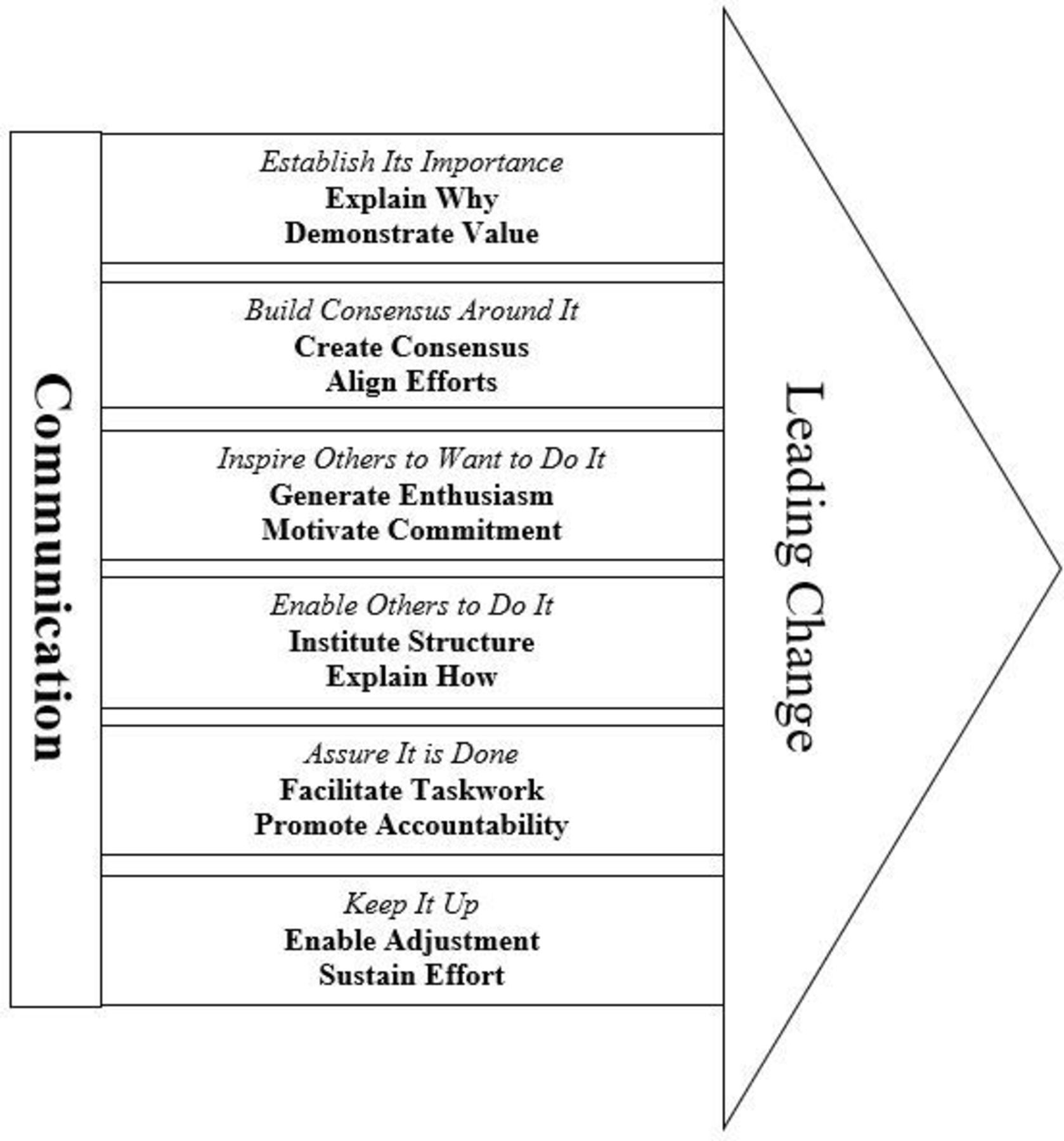
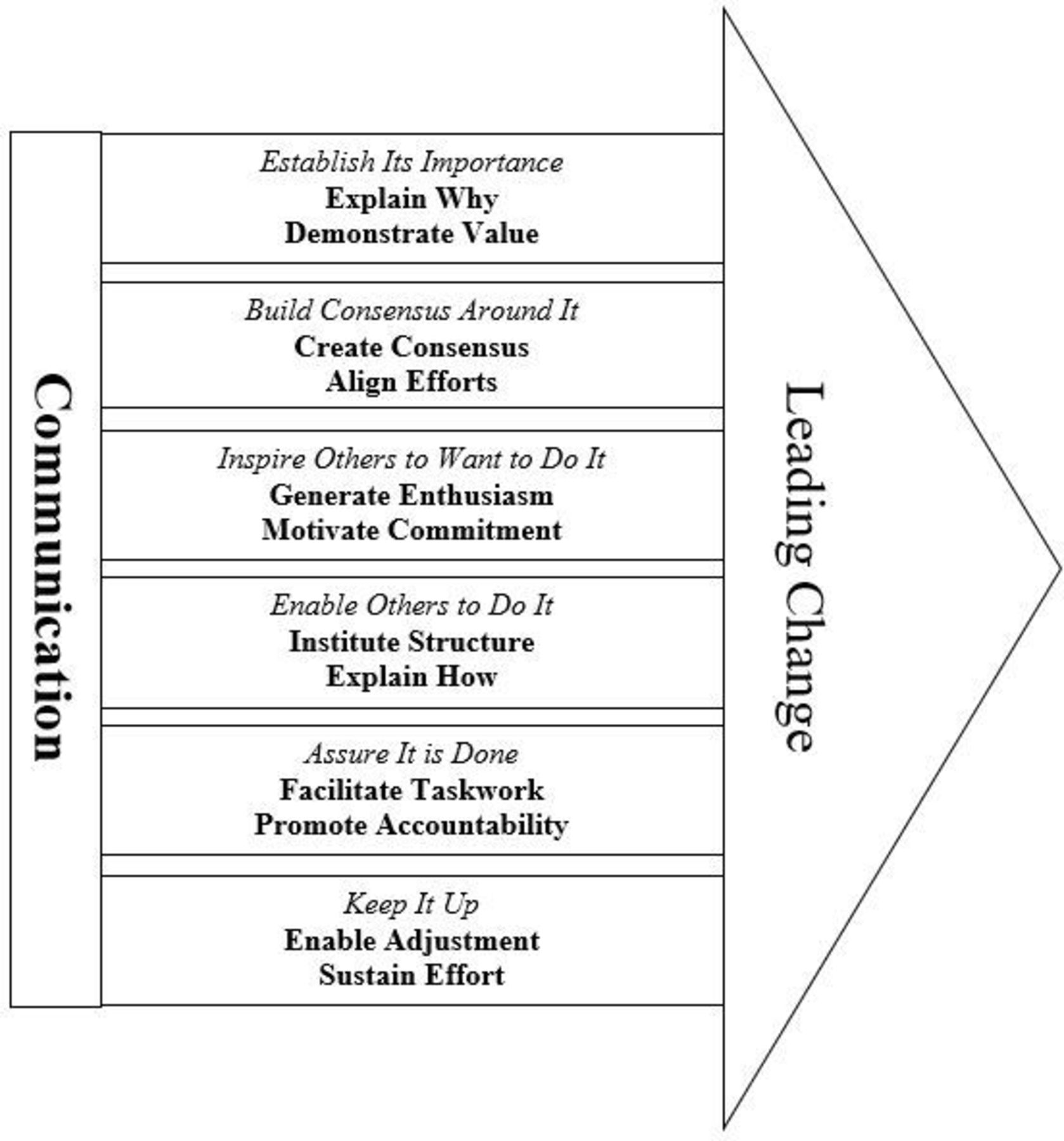
Results Using inductive content analysis, we identified six core pillars of leading change, which are supported by a foundation of effective communication. Within these six pillars, there were 12 functions, including explain why, demonstrate value, create consensus, align efforts, generate enthusiasm, motivate commitment, institute structure, explain how, facilitate taskwork, promote accountability, enable adjustment and sustain effort. Our model offers unique insights on leading sustainable change in healthcare organisations.
Conclusion Using inductive content analysis of semistructured interviews, we have identified 12 important change leader functions and have organised them into a conceptual framework for leading change in healthcare. Individuals involved in leading change initiatives or developing training programmes to help others become effective change leaders can use this framework to ensure they are comprehensively addressing the necessary tasks for sustainable change.
- effectiveness
- improvement
- behaviour
- multidisciplinary
- multiprofessional
Statistics from Altmetric.com
Introduction
The healthcare industry faces strong pressure to improve the quality of patient care in numerous ways. For example, care providers are asked to improve value by reducing delays to timely access of high quality care,1 improving patient recovery following surgery2 and decreasing preventable medical errors.3 4 Prior research has identified several factors that influence the success of quality improvement initiatives (eg, public health policies5; human factors variables6; and gaps in knowledge, skills or abilities7). However, to adopt and sustain any quality improvement initiative, there must be individuals at the forefront, leading the change effort.
Understanding change leader functions (ie, the tasks change leaders should do or assure get done) has become increasingly important, as more hospitals encourage involvement in change initiatives. For example, the MAGNET programme—a programme respected for promoting nurse leadership and improving patient outcomes—explicitly identifies quality improvement as one of the ‘forces of magnetism’.8 Similarly, involvement in change initiatives has become a requirement for many residents and fellows in ACGME training programmes.9
Prior research suggests that a healthcare professional’s ability to implement change is a critical component of what makes an effective leader,10 and that to effectively implement change, healthcare providers must possess the competencies necessary to champion for that change among their colleagues and within their larger organisation.11 As care providers are asked to become change leaders, it is critically important to uncover what functions/tasks are required of care providers outside of their traditional job tasks (eg, patient care). However, there is little guidance on this topic. Accordingly, the present research effort focuses on identifying the functions involved in leading change and organising them into a conceptual framework.
Background
Numerous models of change implementation have been offered over the years. In a recent review of structured strategies for best practice implementation in healthcare, four models were identified as having widespread applicability: (1) Promoting Action on Research Implementation in Health Services (PARIHS); (2) reach, effectiveness, adoption, implementation and maintenance (RE-AIM); (3) knowledge-to-action (K2A); and (4) Consolidated Framework for Implementation Research (CFIR).12 Although these four models of change implementation all address important elements relevant to change, none of them provide sufficient depth on the process of change implementation from the perspective of the individuals leading the change effort to help individuals be successful change leaders.
There have also been several studies of change leaders in healthcare organisations. Some scholars have explored capabilities such as emotional intelligence13 or competencies, such as measurement of intervention outcomes.14 Other studies discussed elements that acted as barriers to change, noting that clearly defined competencies (eg, collaborative change management, life-long learning, visionary) were a central component to optimising leader effectiveness.15 However, these studies focused on a small set of competencies or capabilities (ie, what change leaders should know), rather than functions (ie, the tasks change leaders should do). By adopting a behavioural approach to change leadership, we endeavour to provide an actionable framework, minimising challenges experienced in the knowing–doing gap.
Method
A study review was completed by an institutional review board before launch. The material for this study was gathered through semistructured interviews with 31 healthcare providers employed by a large cancer care hospital in the USA. A purposeful sampling strategy was used to select and recruit individuals from different positions within the organisation who were especially knowledgeable about our phenomenon of interest; successful quality improvement initiatives (ie, met or exceeded the stated objectives in their project proposal).16 All quality improvement initiatives featured in this study were care provider driven (eg, implementing changes in patient pathways to enhance patient recovery), in contrast to top-down externally driven initiatives (eg, compliance with changes in regulation). Potential interviewees were contacted by email containing information about the research topic and study procedures. Approximately 75% of individuals who were contacted for an interview agreed to participate in the study. The interviewees held multiple different positions: 3 surgeons (10%); 4 anesthesiologists (13%); 8 certified registered nurse anaesthetists (26%); 3 advanced practice providers (APPs) (10%); 3 nurses (10%); 1 dietician (3%); 2 project consultants (6%); 2 research coordinators (6%), 2 administrators (6%), and 3 information and technology (IT) personnel holding management positions (10%). This diverse sample helped garner insights into leading change in the context of quality improvement initiatives in a more comprehensive manner by incorporating a broad range of perspectives. During the first round of participant solicitation, theoretical saturation was reached, indicating an appropriate conclusion to sampling.
The interviews were conducted at the cancer centre between November 2017 and February 2018, and lasted on average 29 min (SD=11). All participants consented on arrival. To encourage deeper disclosure and a sense of confidentiality, all interviews were conducted by two of the authors who both have positions at academic institutions external to the organisation. The interviews were structured to elicit functions needed to effectively lead change. To help ensure comprehensive capture of the conceptual domain, participants were first asked to discuss a specific quality improvement initiative (eg, Describe the initiative; what specific things did each person involved in the initiative do? Looking back, is there anything else that should have been done?) and then were asked about their insights on the functions required to lead change more broadly (eg, could you list up to 10 functions that you believe were most important to the change initiative? If a colleague was about to launch his/her first change initiative and asked you what it takes to be an effective change leader, how would you respond?). Most of our interviewees had been a part of numerous successful change initiatives and were able to draw broadly from their knowledge and experiences.
The interviews were audio-recorded and transcribed. Transcriptions were password-protected, stored on an encrypted personal computer and cleansed of any personally identifying information. An interpretivist paradigm guided data analysis, as this perspective broadly characterises qualitative research taking the epistemological stance that knowledge is generated based on shared beliefs.15 We used content analysis to analyse the semistructured interviews.17 Content analysis is a systematic coding and categorising approach that is suitable for examining textual information as well as useful in determining patterns across a data set.18–21 Following the recommendations set forth by Elo and Kyngäs, our content analysis consisted of three phases: preparation, organising and reporting.18 These phases provided a structure to ensure that coding occurred systematically, thus promoting rigour, transparency and replicability. We comment on each of those phases as follows and provide additional information on our methods in box 1 and table 1 .
Data analysis
Step 1: data immersion with subject matter expert (SME)
Lead researcher read through all transcripts before line-by-line coding.
SME read through randomly selected transcripts.
Meeting was held between the lead researcher and SME to reach consensus.
Step 2: determined unit of analysis and manifest content with SME
Meeting was held between lead researcher and SME to discuss the conceptual landscape.
Both lead researcher and SME determined the unit of analysis.
Both lead researcher and SME determined the form of construct manifestation.
Step 3: developed organisational structure with SME
Developed a system of organisation by creating code sheets in Excel version 16.39.
Each section of interview questions within the protocol had a corresponding sheet in Excel dedicated to capturing and organising the data.
Each sheet was labeled with the study ID, job role, department, interviewer, date, coder, quality improvement initiative role and initiative success (the interviewee descriptors).
Step 4: SME consensus coding
SME and lead researcher met and coded three transcripts to develop theoretical and contextual sensitivity.
Step 5: initial coding
Lead researcher and trainee each open coded one transcript, independently creating pithy categories reflective of each response statement.
Lead researcher and trainee met to discuss differences until consensus was reached.
Transcript coding continued with consensus meetings after the third and sixth transcripts were coded.
Lead researcher integrated any changes made to the codebook across all transcripts.
Step 6: data categorising with SME
Lead researcher and SME met several times.
Discussed all coding pertaining to functions.
Analysed pithy categories into more distinct first-order categories.
Organised pithy categories into second-order categories.
Organised second-order categories into main categories (core function).
Identified the six overarching themes and developed the initial conceptual framework.
Created table to reflect data structure in excel sheet.
Together created descriptions for each core function.
All category codes were added to the code sheets.
Step 7: member checks
Lead researcher and SME shared initial findings with two key informants to assure interpretive and descriptive validity.
All discrepancies were discussed until consensus was reached.
Techniques to enhance Trustworthiness in data collection and analysis
Preparation
The preparation phase involved being immersed in the data, getting a sense of the entire conceptual space, selecting the unit of analysis and deciding whether to analyse manifest or latent content.18 Accordingly, two authors immersed themselves in the data by reading the transcripts from all the interviews. In general, the sentence was selected as the unit of analysis. Using sentences preserved the context of the phrase, whereas single words would have been too narrow and entire question responses may have been too broad. However, the question which prompted the interviewee to list multiple functions necessitated using the word as the unit of analysis. For the initial codes, we focused on manifest content. This approach is consistent with open coding in the inductive approach, which is later grouped, categorised and abstracted to more latent constructs.18
Organising
The organising phase involved conducting open coding and creating categories at the specified unit of analysis, grouping those codes under higher order headings (more generic categories) and then abstracting the main categories.18 During the open coding, notes and headings were written in the text while reading it, using as many codes as necessary to describe the content. The codes were then copied from the transcripts to a coding sheet and grouped into higher-order headings.22 This reduced the number of codes from 332 to 120 first-order categories, which were then grouped into 60 second-order categories. In this process, careful attention was taken to keep in mind ‘that creating categories is not simply bringing together observations that are similar or related; instead, data are being classified as ‘belonging’ to a particular group and this implies comparison between these data and other observations that do not belong to the same category’.17 The 60 generic categories were then grouped into main categories (12 core functions plus communication), naming them using content-characteristic words.22
Reporting
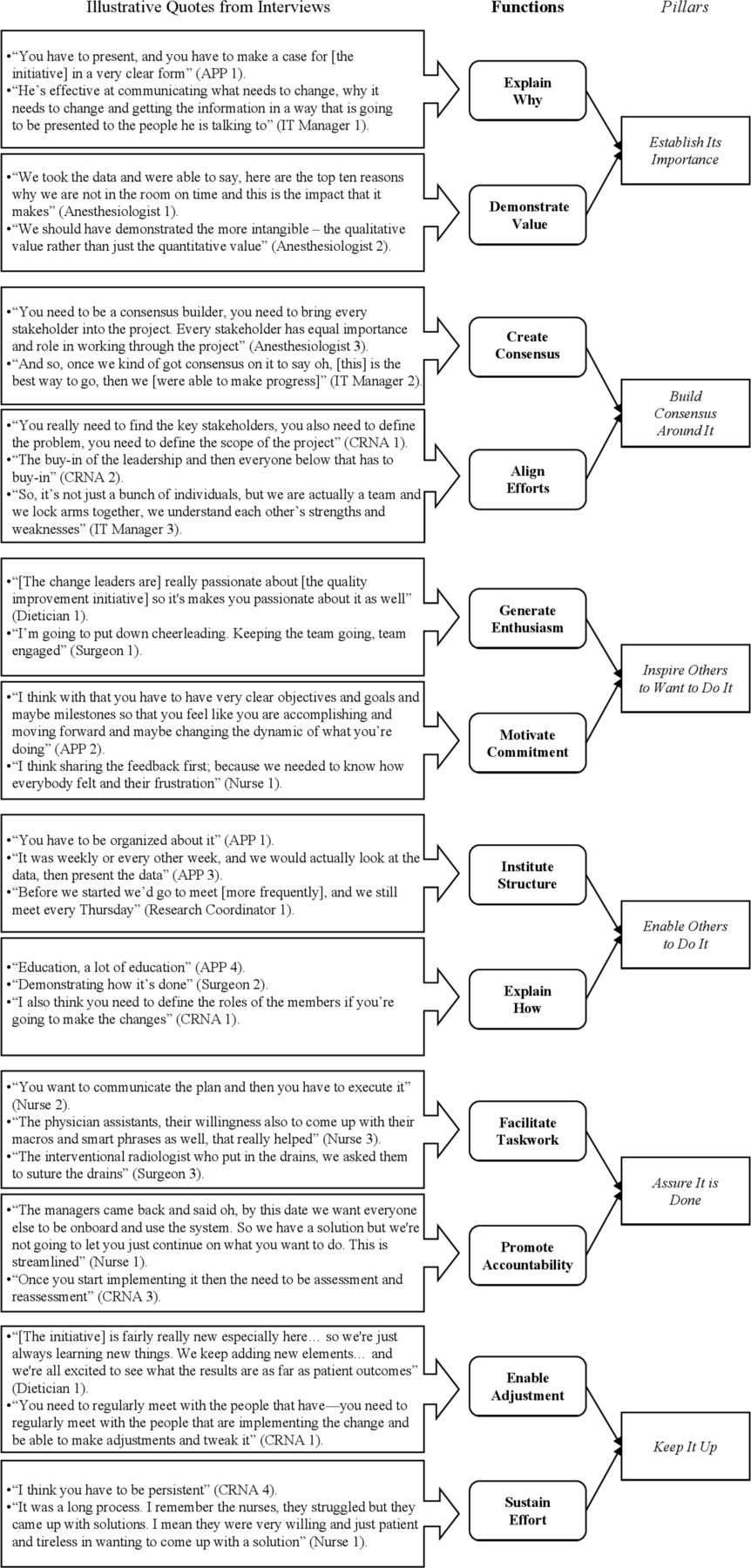
For qualitative content analysis, the reporting phase typically involves reporting the analysing process and the results through conceptual models, maps, categories or story lines.18 We first present our data structure in figure 1, followed by our overarching conceptual model in figure 2.

Change leader pillar data structure. APP, advanced practice provider; CRNA, certified registered nurse anaesthetist; IT, information technology.
{kind=link}
{kind=link}
Conceptual framework of change leader functions
Results
Twelve core change leader functions emerged from the data. A pattern also surfaced across the functions, making it clear that they should be organised into six overarching themes—or pillars of change leadership. Each pillar contains two functions. Notably, the first function lays the foundation for the second function. As the change process is non-linear and requires numerous adjustments both prelaunch and postlaunch, effective change leaders must be able to iterate between the functions and pillars at each stage (ie, before, during and after launch).
All pillars are based on a foundation of effective communication, which emerged and impacted the entire set of functions. Interviewees expressed the critical role of communication both across levels (eg, ‘communicating is the key to a lot of, to any project, … your ability to communicate upward for executives and communicate downwards as well, is critical’, project consultant 1) and throughout the change implementation process (eg, ‘communication throughout obviously, just initially with us two and then collaborating with other outside experts’, APP 4). As several different quality improvement initiatives were noted by the interviewees, we use the term ‘it’ to refer to the quality improvement initiative to increase readability.
The first pillar, establish its importance, contains the functions of explain why and demonstrate value. Explain why involves communicating the initiative’s vision and purpose, as well as translating that vision into overarching objectives that will help steer the initiative. Stated differently, ‘the why, why is it that we’re going to do this’ (IT manager 3). Demonstrate value involves illustrating the impact of the change, ideally on multiple different outcomes. Early in the change process, this may be anticipated value (eg, comparing internal performance to national performance to demonstrate room for improvement), whereas later in the change process, it is actual value. Several interviewees emphasised the importance of data for demonstrating value (eg, ‘evidence and data are important for change’, anaesthesiologist 1), whereas others noted the importance of demonstrating value beyond financial outcomes (eg, ‘demonstrating value, and not just leaving that value as monetary’, anaesthesiologist 2). Together, the functions of explain why and demonstrate value enable sustained change by establishing both the anticipated and actualised importance of the change initiative.
The second pillar, build consensus around it, focuses on the functions of create consensus and align efforts. Create consensus involves developing a shared understanding and generating agreement. Consensus was discussed both broadly in terms of agreement in general (eg, ‘For me I think a consensus is better because you’re more likely to have everybody on board to help you out and to accomplish the change that you want to see’, APP 2) and in terms of agreement on specifics (eg, ‘To measure what our on time starts were, we had to come to an agreement, a definition on what was an on time start’, anaesthesiologist 1). Align efforts involves identifying key stakeholders and generating buy-in for the initiative. One interviewee noted: ‘You can’t enact any change or realise any vision unless you have the right people on the bus in the right seats’ (administrator 1). Effectively creating consensus upfront makes it easier to align efforts later.
Alternatively, the third pillar, inspire others to want to do it, includes the functions of generate enthusiasm and motivate commitment. Generate enthusiasm involves demonstrating passion and inspiring interest, which one interviewee expressed as ‘you need to be passionate about it, you really believe in it, and that you feel it will make a difference and will make an impact, then others follow’ (APP 1). Motivate commitment involves setting goals (eg, ‘so of course, you have to have a goal first’, nurse 2) and providing feedback—especially when it acknowledges the value of contributors (eg, ‘a leader makes all members of the team feel included, a leader makes everyone feel important, a leader motivates followers’, dietician 1). Conceptually, generating enthusiasm creates that initial spark of interest, whereas motivating commitment turns that spark into a fire.
The fourth pillar, enable others to do it, encompasses the functions of institute structure and explain how. Institute structure involves determining how work will be accomplished, and instituting mechanisms to facilitate shared understanding. For example, ‘I make an agenda and send it out to everybody, so it helps organise those meetings‘ (research coordinator 2). The explain how function involves education and instruction on the quality improvement initiative’s technical elements. The importance of education was raised numerous times in our data, such as ‘Education. It’s also so important because you have to communicate with them what they have to do’ (research coordinator 1). Instituting structure generates the shared understanding necessary to create clear and consistent instructions, which enable effectively explaining how.
The fifth pillar, assure it is done, includes the actual taskwork required to carry out the initiative as well as the promotion of accountability. The facilitate taskwork function focuses on carrying out the components of the change initiative (eg, ‘We had nurse navigators and they would call patients after they were discharged’, surgeon 3), as well as proactively removing barriers to taskwork (eg, ‘if you’re planning, before it goes into action, the most important part is trying to forecast potential challenges and proactively formulate solutions’, dietician 1). Alternatively, the promote accountability function focuses on assessing compliance and holding appropriate parties responsible (eg, ‘But also I think like some—like a system that holds people accountable. Like you know when we had a—like 2 month of actual audit where like we checked on everyone’, surgeon 2). Upfront efforts to facilitate taskwork help ensure high change adoption rates, which makes promoting accountability easier.
Finally, the sixth pillar is the sustainability pillar titled keep it up. This pillar involves the functions of enable adjustment and sustain effort. Enable adjustment involves efficiently making changes in response to new or changing circumstances, as well as identifying and enacting solutions for problems. One of the interviewees expressed, ‘Just an understanding that this is an ever-changing process, and as things develop we need to be adaptive to it’ (APP 5). Similarly, the sustain effort function encapsulates components that are put in place or actions that are carried out to sustain the change initiative over time—even in the presence of resistance. This encompasses the resilience and perseverance needed to follow through with change. Stated differently, ‘It’s a recognition that in the journey, you may have sometimes where you fall down but you get back up, and you keep going’ (IT manager 3). Although these functions are both essential later in the change process, they are also important in the prelaunch stage as navigating and sustaining through all of the change preparations takes a lot of effort. Early in the change process, change leaders should incorporate enabling adjustment into their plans as it helps to avoid the change battle fatigue that hinders sustaining effort.
Each pillar appeared in our data numerous times, ranging from 12% to 25% of all sentences and words coded. Inspire others to want to do it appeared most frequently (25%), followed by establish its importance (21%) and enable others to do it (16%). Assure it is done and keep it up each had 13% of codes, followed closely by build consensus around it with 12%. Although the goal of theoretical sorting is not to produce symmetrical categories,22 the numerous examples attributable to each pillar gives us confidence that each pillar is sufficiently important to warrant a change leader’s attention and inclusion in our framework.
Discussion
Our study revealed numerous insights about change leader functions in a healthcare organisation. Extending functional leadership theory23 the current endeavour explicitly considered leadership in the context of quality improvement implementation. The literature surrounding leading change has supported the critical need for strong leadership as a key element to champion change and implement the quality and safety initiatives necessary to transform healthcare. However, research on the specific actions involved in leading change initiatives had yet to be examined. The present endeavour identified 12 functions critical to leading change in healthcare, as well as an organising framework (see figure 2). In contrast to other models of change implementation (eg, PARIHS,24 RE-AIMS,25 K2A26 and CFIR27), we present an individual-focused framework for change implementation that highlights interactions with the change recipients, is specific enough to be actionable and extends beyond the initial implementation to consider sustainability. This framework has implications for care providers to use for their own personal development as well as educators to use as a blueprint for formal training content. By improving healthcare personnel’s ability to effectively lead sustained change it sets the foundation to enhance the quality and safety of patient care.
Notably, our functions have some conceptual similarities to and differences from several classic leadership theories. For example, two of the most robust leadership concepts are consideration and initiating structure, the latter of which is similar to our functions of institute structure and align efforts.28–30 In addition, transformational leadership involves the four elements of inspirational motivation, individualised consideration, intellectual stimulation and idealised influence.31 32 Although transformational leadership focuses more on the leader’s interactions with followers in daily activities, the shared emphasis on inspiration and motivation present in our pillar of inspire others to want to do it is noteworthy. Empowering leadership likewise has multiple factors with some conceptual similarity: leading by example (facilitate taskwork), participative decision-making (create consensus), coaching (explain how) and informing (explain why).33 34
Turning to key differences, the most noteworthy extensions provided by our model relate to sustaining the change effort. More specifically, in each pillar, the first function sets the foundation for the second function, and together they promote sustained change. For example, in the first pillar (establish its importance), whereas it is certainly important to explain why, without its companion function of demonstrating value, this pillar would fail to promote sustained change. Whereas care providers may readily agree with the ‘why’ of improving patient safety, given their high work demands, demonstrating value sustains efforts by showing that the efforts are worthwhile (eg, patient falls have been reduced by 50%). Without such a demonstration of value, the behaviours are likely to extinguish as care providers turn their attention to other job requirements or other quality initiatives (eg, reducing infections). The sixth pillar (keep it up) also provides the common insight that continued effort is necessary (sustain effort), with a unique companion function of enable adjustment. Enable adjustment highlights that the original initiative will require ongoing adaptation as problems are uncovered or new evidence becomes available. Simply sustaining effort can result in a great deal of effort in the wrong direction, thus combining it with enabling adjustment is required for sustainable success. Thus, our conceptual framework provides unique insights into the companion functions that enable change leaders to set themselves up for success while acknowledging that change is a non-linear process that requires revisiting each pillar at each stage—whether to plan for or enable action.
This study used qualitative methodology in a field setting. This approach strengthens the external validity, yet as all participants were from one organisation, it also presents the opportunity for confounding variables (eg, structure and culture). In addition, we deliberately sampled broadly across a variety of roles to capture multiple perspectives. However, the majority of these roles were related to surgical oncology (21 of 31 interviews), and it was beyond the scope of the present investigation to examine all roles within the organisation. Finally, the use of interviews enabled capturing a broader array of potential functions as experienced by the participants; yet, as each participant only participated in one interview, our insights are limited by their retrospective reports of their experience.
Future research should consider a multicentre longitudinal qualitative investigation, observing and interviewing change leaders throughout the change process. In addition, a robust quantitative investigation of potential differences in function importance between roles/positions across multiple types of care settings may yield important insights. Finally, we hope future research will develop a training programme based on our model and test its efficacy in a field-based experiment with multiple data collection points.
Effective change implementation is the enabler of improving quality and safety in healthcare organisations. The present effort has established the key functions that healthcare leaders should carry out to promote effective and sustained change. Notably, our six-pillar framework addresses the need for a comprehensive individual-focused framework for leading change that is specific enough to be actionable and addresses the interactive nature of leading change. The functional nature of the framework holds many implications for both research and practice, lending itself to both empirical investigation and immediate usage by care providers.
Acknowledgments
The authors acknowledge the support and advice of Margaret Beier and Fred Oswald, from Rice University, whose valuable input helped refine and improve this work. The authors also wish to acknowledge Minh-Hue Mosley, from the University of Texas MD Anderson Cancer Center for her administrative support.
References
Footnotes
Contributors ALW, MML, TAA, VG and ES provided substantial contributions to the conception of the work and interpretation of data. TAA recruited the sample. ALW and MML conducted the interviews, led the analyses and drafted the paper. TAA, VG and ES provided feedback and revised the manuscript critically. All authors approved the final manuscript. ALW is guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was granted by the Rice University Institutional Review Board (IRB-FY2018-204).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Interview protocol is available upon request from the first author. Complete interview transcripts are not available to protect interviewee confidentiality.