Article Text

Abstract
Purpose There is growing interest in the potential need for clinical involvement in leadership and management of hospitals. Most studies of clinical leadership use US and European data. This paper contributes the first evidence for the country of Iran. It examines three different forms of hospital system: public, private and social security organisation, and these include teaching and non-teaching hospitals. This study adds to a small but growing literature that examines the possible value of ‘expert’ clinical leaders.
Method This study uses data from 72 general hospitals in the city of Tehran. The data were collected for years 2015 and 2016. Data Envelopment Analysis is used to assess hospital performance. Hospitals’ chief operating officers are divided into two groups: clinicians, the majority of whom are physicians (doctors), and non-medically trained managers.
Findings The average performance scores for hospitals with clinical managers and non-clinically trained managers are equal to 96.68±5.50 and 89.78±7.20, respectively (p<0.001). Performance is thus higher under clinical managers. Outcome differences are observed in each of the three types of ownership and in teaching and non-teaching hospitals. The advantage in performance-score varies, when comparing the clinically led institutions and managerially led institutions, by between 5 and 10 points on a 0–100 scale. These differences remain after regression-equation adjustment for other influences.
Practical implications Succession planning and targeted leadership development is made more efficient with greater awareness about the kinds of leaders and managers that enhance organisational performance.
- clinical leadership
- engagement
- medical leadership
Statistics from Altmetric.com
Introduction
Interest in clinical leadership is continuing to grow. In the academic literature, five distinct but linked areas appear to have emerged. Each takes a different approach.
The first adopts an internal perspective. By developing a medical engagement scale (MES), Spurgeon and colleagues (2011) were able to assess the influence of clinical engagement—expressed simply as having a high level of organisational commitment.1 The authors found, in a number of studies, that enhanced clinical engagement is positively associated with organisational performance across a range of measures.2–5 A second body of work, which adopts a similarly internal focus, examines the challenges clinicians face as they bridge the dual identity of ‘professional’ and manager.6–8 As clinical executives have grown in influence so too have the hybrid manager–professionals.7 This dichotomy is acknowledged and incorporated into the third body of literature that examines how best to develop clinical leaders; these studies seek increasingly to align leadership programmes with measurable outcomes.9–14 The clinicians in our study seem unlikely to have received professional leadership training.
The two remaining themes of research attempt to assess clinical involvement at the governance and Chief Executive Officer (CEO) level. In a review article, Sarto and Veronesi (2016) found that more studies examine participation at the board level, and US data are most common, which partially explains why studies on private hospital systems dominate.15 Although this work is mainly cross-sectional in design, it suggests that clinical, particularly physician, presence on hospital boards is predictive of better hospital performance.15–18
The final body of work, into which our study falls, attempts in a simple way to correlate hospital performance scores with the prevalence of clinicians as CEO, as compared with non-clinically trained managers who occupy these positions. Since the 1980s, the ‘merits’ of clinical leadership have been championed; however, real evidence was lacking. As an attempt to make a start, Goodall (2011) posed the question, are hospitals ranked higher in ‘US News and World Report Best Hospitals’ ranking’ when they are led by a physician or a non-medically trained manager? The study revealed a statistically significant relationship; quality scores were found to be 25% higher in physician-led hospitals.19 A more recent study advanced this approach and examined whether hospital systems led by physicians were associated with better quality ratings, financial performance and operating efficiency compared with those led by non-medical managers.20 Tasi and colleagues (2018) found that physician-led hospital systems had higher quality ratings across 12 medical specialties and they had more inpatient days per hospital bed than did non-medically led hospitals. Interestingly, they found no differences in the total revenue or profit margins between the groups.20 The review by Sarto and Veronesi (2016) suggests that the direction of evidence appears to support the claim that clinical involvement in leadership has a positive influence on hospital performance outcomes (eg, financial, operational, quality of care, mortality).15
While studies across each of these five areas are mounting in number, there are noticeable gaps that remain. In particular, research on clinical leadership from health systems beyond the USA and Europe is largely absent.
This paper attempts to make a start. In modern data from Iran, we ask the question: is there evidence that performance scores are higher in hospitals where the senior executive is a clinician compared with those managed by a non-medical manager? A second contribution made possible in this study is to compare across three different healthcare systems: private, government and not-for profit, and among teaching and non-teaching hospitals.
Significance for leadership research
The focus in our study is on senior executives. Following Spurgeon and colleagues (2015), we believe the deliberations about manager versus leader are somewhat spurious.4 Not all middle managers will have the capacity or desire to become an executive leader, but most leaders will have been managers at some stage in their career.
Those in leadership and management positions command huge resources and they make decisions that affect the lives of all employees. Line-managers have a significantly larger influence on employee job satisfaction than does their pay; double the effect.21 Our setting in this study is healthcare. However, we believe it is important to look for patterns beyond a single work place setting and to aim, as an ideal, for generalisability where possible. In the discussion section below, the relevance of our finding will be assessed with reference to the literature on medical engagement and expert leadership. We will draw from the extant literature to raise suggestions about why in healthcare, clinical leaders may be associated positively with organisational performance.
In the next section, we outline our methods; we summarise our data and our statistical analysis. Unlike in previous studies that use hospital rankings,19 20 we use two different measures of hospital performance.
Methods
Hospitals in Iran
There are 924 hospitals in Iran (see table 1). These are mainly administered by three bodies: the majority (570) are owned by the Government’s Ministry of Health and Medical Education (MOHME). They are classed as public and include teaching and non-teaching hospitals.22 Public hospitals are funded by government, partially through health insurances. Most budgetary, human and capital investment decisions are made centrally by civil servants in government. The medical universities determine the local strategic priorities for each hospital.
Hospitals in Iran*
The Social Security Organisation (SSO), which is a non-governmental organisation (NGO), runs 70 hospitals in Iran. The SSO provides various welfare services including retirement benefits and disability pensions and provides healthcare services for insured people. The SSO also delivers hospital-based care, through hospitals that it owns and operates and by purchasing services from other providers. SSO hospitals are funded directly from insurance payments with minimal local autonomy, like public hospitals.23
The second-largest group of hospitals in Iran are those owned by the private sector (152). Private hospitals are run by a board of trustees composed of their main shareholders; they are autonomous in terms of cost and revenue and in terms of recruitment. Our study focuses only on MOHME, SSO and private general hospitals in one major city, Tehran.
Hospitals in the study
Our data include 72 general hospitals located in Tehran; 44 are public hospitals administered by MOHME, 13 belong to SSO and 15 are privately run hospitals. They are evenly divided between teaching (35) and non-teaching hospitals (37). The mean number of beds per hospital is 231 (SD=143). Information on each hospital has been obtained from the Annual Statistical Report published by the Universities of Medical Sciences in Tehran or directly from the MOHME.
Minor differences exist in the administration of hospitals run by each of these bodies. Physicians sit in the most senior leadership positions in most hospitals; this role, hospital director, is mainly medical and it reflects the status of physicians in the Iranian healthcare system. MOHME as the main custodian and Medical Council is highly influential in macro health policy; it is led by physicians.24
The hospital director—the most senior physician—is head of the medical staff, chairs hospital committees, is technically and legally responsible for the provision of medical services and is expected to manage relationships with external bodies including government and the associated university. The hospital director has minimal direct powers associated with the position in areas such as financial or operational matters, or in human resources. Thus, directors are not involved in the day-to-day management of hospitals. In public hospitals, the appointment of director is made by the medical universities, and in private institutions, governing boards select the lead physician. The administration of nursing staff in all hospital systems is led by a nurse matron.
Chief operating officer (COO)
The physician hospital director delegates responsibility for administration to a COO. In public, private and SSO hospitals, it is the COO who holds executive responsibility for financial and operational performance, and the general management of hospitals. Decision-making about strategy, human resources and investment planning is shared between the COO and the board of directors in private hospitals. COOs, in public hospitals especially, tend to work within the boundaries of the ‘authorising environment’.25 The COOs in our study have on average 11.91±2.92 years of experience in a senior management role and they include and clinicians and non-medically trained managers.
As in previous studies,19 20 data were collected via hospitals’ websites, and when information was incomplete, direct contact was made. Each of the 72 COOs is categorised into one of two groups: clinician COOs which include physicians (doctors), nurses, midwives, anaesthetic technicians and those who are non-clinically trained managerial COOs (see table 1). There are 35 physician COOs and six COOs who include nurses, anaesthetic technicians and midwives. Thus, there are 41 clinically trained COOs among the 72 (56.9%).
Non-clinically trained managerial COOs (31) consist of graduates in healthcare management, public management and accounting. To be included in our data COOs must have at least 2 years of senior management experience in their present hospital. Three of the COOs are female. Clinical COOs are more often found in public hospitals (28); there are nine in private hospitals and five in SSO organisations (see table 2). Because the number of non-physician clinician COOs is small (6), it was not possible to compare the effect of this group with physicians. Thus, physicians and other clinicians have been combined.
Description of data
Hospital performance evaluation methods
To perform the statistical analysis, a measure of hospital performance is required. Two main approaches might be considered. One is so-called Stochastic Frontier Analysis (SFA) and the other is Data Envelopment Analysis (DEA).
SFA builds on the economist’s standard notion of a production possibility frontier but adds an externally driven random-error term. Its chief limitation is that it is an inherently parametric approach and is necessarily based on explicit assumptions about the underlying production technology. Some previous literature in health economics has used this method to assess the efficiency of hospitals.26–29 Because the SFA method implicitly requires the construction of an efficient production-frontier function, detailed information on input prices, output prices and other input costs is, in principle, required. For the current setting of Iranian hospitals, such information is not available.
DEA is a feasible and practical alternative. Its advantage is that it requires statistical investigators to have less information about the exact technology in the industry—in this case, the health sector being studied. DEA offers a non-parametric method for the analysis of production functions and can be thought of akin to a way of understanding a best-practice frontier (rather than the theoretically ideal frontier). DEA is a linear-programming methodology for evaluating the efficiency of each production unit among a set of fairly homogeneous decision-making units.
The approach of DEA is to view a production possibilities frontier (a data envelopment or efficient frontier) using combinations of inputs and outputs from best performing hospitals.28 29 Thus, we define a
This is a simple technique that, consistent with intuition, views favourable hospital outcomes as being ones with a high ratio of outputs to inputs.
DEA is used in this study to calculate a measure of the performance of the sampled hospitals. Performance data were collected from three medical universities in Tehran (Tehran University, Iran University and Beheshti University). We adopt an input-oriented DEA model in which hospital COOs are assumed to have some control over their inputs (personnel, beds and operating expenses) when faced with imperfectly controllable demand factors and outputs (such as the number of in-patients or out-patients). The model effectively focuses on the desirability of the minimisation of inputs with given outputs, with the character of an efficient non-profit organisation. Some previous empirical research has used an input-orientation model for the evaluation of hospital efficiency.26–29 These were used to guide our selection of variables.26–29
The inputs include three broad categories: labour (eg, human resources), materials (eg, drugs) and capital (eg, buildings and equipment). Variable selections generally follow the representativeness, measurement convenience and availability of data.30 In this paper, the number of physicians, nurses and other personnel (people of pharmacy department, clinical laboratory, medical imaging department, radiology department and other medical auxiliary departments) and the number of beds (as a proxy indicator for capital inputs) are selected as ‘input’ variables; the number of outpatients, emergency visits and inpatient days are selected as ‘output’ variables.31 32 (These input and output variables are listed in table 3.)
Definition and measurement of variables
Hospital performance was computed using the DEA method with standard software package DEAP V.2.1 (the achieved scores from the software range between 0 and 100). An average of hospital performance in 2014 and 2015 is used. Standard statistical methods are followed, including t-tests and linear regression equations.
The central focus here, as in studies such as Goodall (2011) and Tasi et al (2018),19 20 is a comparison of the performance of (1) hospitals managed by medically or clinically trained COO to (2) those led by managerial COO who are non-clinicians. The dependent variable in the analysis is the performance of hospitals, and the key independent variable is the nature of management expertise (clinical or managerial).
In the regression-equation model, appropriate statistical adjustment is made for possible confounding influences. The independent control variables used in the analysis are hospital size, the type of hospital activity, the nature of ownership and management length-of-experience. The hospitals were divided into three groups defined as government hospitals, private hospitals and SSO hospitals. We used SPSS V.21 software at a significance level of 0.05.
Findings
Table 3 describes the key aspects of the data set. There are, in total, 72 leaders of hospitals. Of these, 69 are men; 41 of the hospital leaders have a clinical background (35 physicians); 35 are leading a hospital that also does some teaching.
Table 4 illustrates the spread of performance scores across the different hospitals. It reports the mean hospital scores in each of the three sectors covered in this study: public, private and SSO.
Distribution of performance scores for hospitals by ownership type
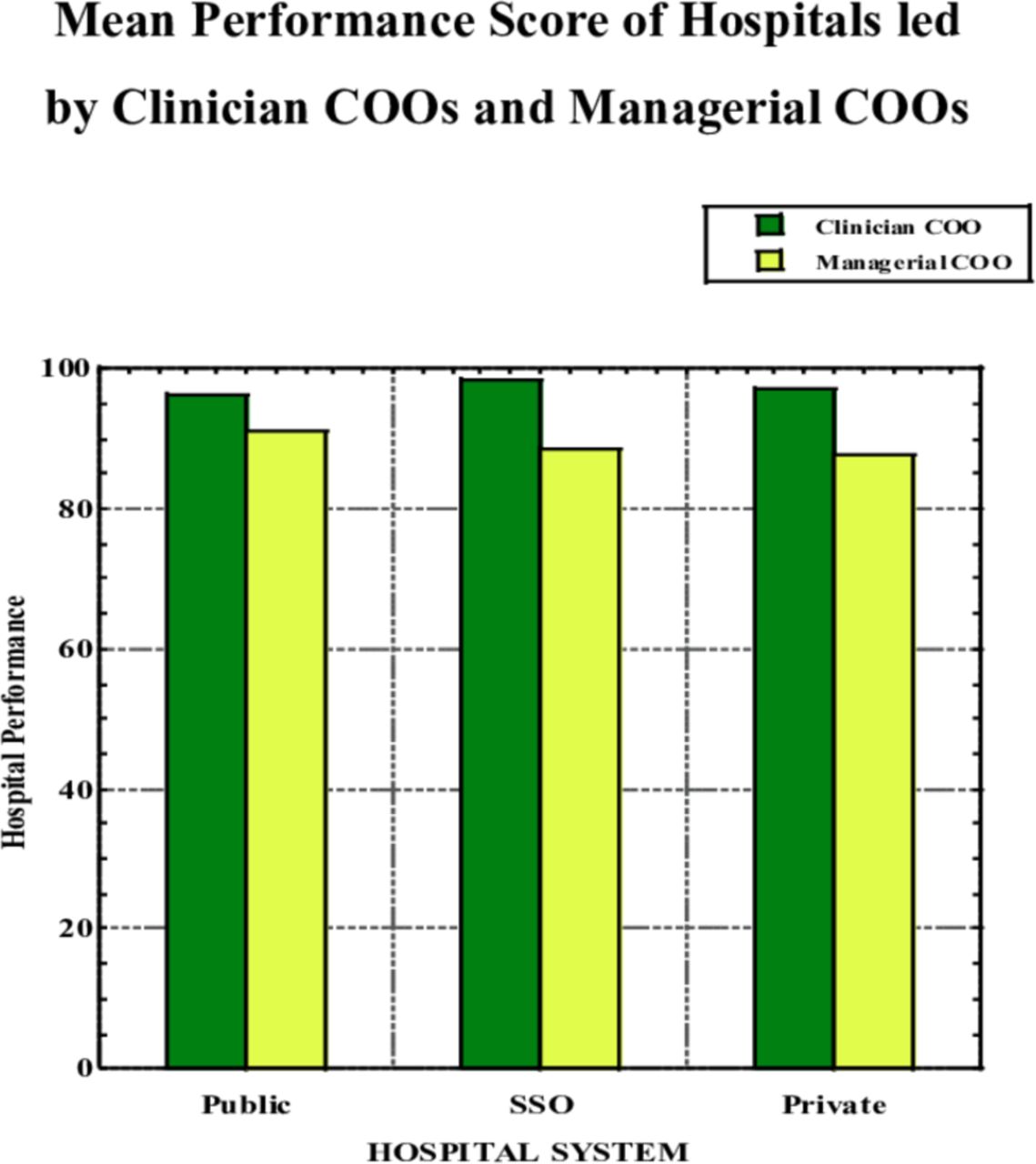
For public hospitals, which are the most numerous kind in the data set, the mean performance of hospitals led by clinicians is 96.18 while that for hospitals led by managerial leaders is 91.12. On a t-test, these are statistically significantly different at conventional confidence levels (the p value is 0.027). Among SSO hospitals, which are the least numerous in the data set, the mean performance of hospitals led by clinicians is 98.31 while that for such hospitals led by managerial leaders is 88.70. Among private hospitals, the mean score of medically led hospitals is 97.32 compared with a mean score of managerially run hospitals of 87.62.
In each of the three categories, therefore, hospitals seem to have better performance scores if they are headed by a COO with a medical background. Moreover, the size of the difference is considerable. The advantage in performance score varies, when comparing the medically led institutions and managerially led institutions, by between 5 and 10 points on a 0–100 scale. These results suggest significant differences between hospitals’ performance based on the nature of the COO’s professional path.
As a more formal test, table 5 sets out regression equations in which the dependent variable is a hospital’s performance score. There are four columns (labelled Model 1 to Model 4). Model 1 begins with the simplest specification and gradually builds up, moving steadily rightwards in table 5, to longer specifications with more independent variables as controls in the equation. It can be seen that the key variable, that for Hospital led by a clinician COO, has a coefficient that is positive and large. It remains relatively stable as extra independent variables are added. The coefficient varies across columns from 6.90 to 5.30. In Model 4, which is the fullest specification, the independent variables are the tenure of the leader, a dummy variable for whether the hospital is a teaching hospital and dummy variables for the type of ownership (whether public, social security or private). The base category for the latter classification is ‘private hospital’. Holding other influences constant, table 5 shows that hospitals have better performance scores when they are led by someone with a long tenure, when they are teaching rather than non-teaching and when they are public. However, among these, only the first is statistically significant at conventional levels.
Multiple regression analysis: Hospital performance equations
The main conclusion from the statistical analysis, and as depicted graphically in figure 1, is that hospitals led by clinicians have better performance scores.

{kind=link}
Represents the mean hospital performance scores for the separate ownership of public, private and SSO based on clinician COO and managerial COO. In each of the three cases, the mean performance score of hospitals where the COO is a clinical graduate is greater than the mean score of the hospitals where the COO is a professional manager. The mean hospital performance score of the public hospitals managed by a clinician executive is 96.18 (SD=6.41), while the mean performance score of public hospitals led by professional managers is 91.52 (SD = 6.83). COO, chief operating officer; SSO,Social Security Organisation.
Discussion
Good management in healthcare organisations is known to positively influence patient outcomes and organisational performance,33 but there is now growing interest in the part played by clinical leaders. Recent evidence suggests that it is not merely engagement but direct involvement in leadership by clinicians that seems to correlate with better performance.1 19 20 34 35 Similar findings are emerging about clinical involvement at board level.16 17 36 However, almost all of the evidence supporting clinical leadership has come from North America and Europe. Our paper extends the literature by focusing on new data from Iran. We perform a relatively simple test to examine whether there is any evidence of an association between hospital performance scores and the kind of leader in charge of the day-to-day running in 72 Tehran hospitals. Our study advances previous work because it allows us to scrutinise the clinical-leader hypothesis in three different hospital systems in one city; these systems include public, private and social security organisation hospitals, and teaching and non-teaching hospitals.
Our Iranian study is a cross-section analysis at one point in time; however, it complements the so-called ‘expert leadership’ literature. This research suggests that organisational leaders and line managers should demonstrate expertise in the core business of the organisation or sector they are leading (eg, a scholar-leader in a research university, a former basketball player as a coach, etc). This pattern— of experts outperforming non-experts in leadership positions—has been replicated in various different settings, at the senior executive level,37–39 at head of department level40 and among government ministers.41 These studies often use longitudinal data with adjustment for confounding variables.
Although there are noticeable variations between institutions and sectors, healthcare undoubtedly shares features with other organisational settings. That the expert-leader finding has been replicated in healthcare and other kinds of work places arguably helps to demonstrate this. As suggested earlier, it seems important when researching the subject of leadership and management to try to identify common patterns across industries.
What might explain the expert clinical leader finding?
Our study finds that the highest-performing hospitals in the Iranian city Tehran are statistically more likely to be led by clinicians—mainly doctors. It complements previous research.15 19 20 It is not possible with this kind of study to address the issue of how clinical leaders might influence performance. However, two areas of research may be able to shed some light. The first points to the medical engagement literature.1–3 5 Spurgeon et al define medical engagement as ‘the active and positive contribution of doctors, within their normal working roles, to maintaining and enhancing the performance of the organisation, which itself recognizes this commitment, in supporting and encouraging high quality care’.1 The MES was developed to assess levels of engagement across different healthcare systems. Spurgeon and colleagues (2015) contend that ‘medical leadership is in itself a mechanism or process to achieve greater medical engagement in the running of the organisation, and that it is this engagement that has the impact upon organizational performance’ (p 177).4 The authors (Spurgeon et al) summarise the engagement literature: they report that medical engagement is necessary to the implementation of important changes and improvements in health systems4; engagement is found to correlate with performance and innovation42; finally, clinicians who were more engaged were significantly less likely to make mistakes43 and more likely to have direct input into the financial bottom line of hospitals.44
The second field of work that may help to inform our findings is the expert-leadership literature. For example, Artz et al. found a strong association between the presence of an ‘expert leader’—who is a line manager—and high employee job satisfaction.21 The workplace data in that study include information on employees from all industries and sectors, including health. Experts are categorised there in three ways: when employees were managed by a supervisor who could perform the employee’s job; if the line-manager worked his or her way up the company or started it and a supervisor’s level of technical competence, as judged by his or her employees. All three of these were predictive of substantially greater levels of job satisfaction among employees. High levels of worker well-being are also known to increase employee creativity and problem solving and raise levels of work engagement.45 46 Employee job satisfaction has also been shown to increase individual productivity in a randomised control trial.47 While it is not possible to directly link our Iranian finding to claims about the benefits of medical engagement, job satisfaction or expert leadership, it seems likely that these factors may play a role. Arguably, the COOs in our data will have had a major influence on the working lives of the medical staff they oversee.
Implications for practice and future research
The studies on clinical leadership and the research findings on expert leadership have practical implications for organisations and healthcare settings. This line of work is immediately translatable to non-academic practitioners and HR managers and can be applied through human-resource processes. Succession planning for line managers and the adoption of a targeted approach to leadership development are made possible with greater awareness about the kinds of leaders that may enhance organisational performance in healthcare.
Longitudinal research will be required in the future to advance our causal understanding about clinical leadership and organisational performance. New research is underway examining how clinical leaders affect employee job satisfaction and intentions to quit—specifically, the practices employed by expert physician and clinician managers.
Limitations
Although our study results indicate that there is a positive association between clinical leadership and the performance scores of Tehran hospitals, we cannot presuppose a causal relationship. As suggested above, to fully establish whether hospitals perform better under clinical leaders will require more detailed performance metrics and longitudinal data, where we can also examine the change in leaders, and the later change in hospital performance. Reverse causality is always a possibility in a cross-section study; better hospitals may choose to hire chief operating officers who have a medical background. Two factors may somewhat weaken this claim, however. First, in our data, each COO has been in place for a minimum of 2 years. Thus, some time in post has been witnessed prior to our analysis. Second, better hospitals are more likely to have a greater choice in their selection of senior staff, because working in successful organisations is likely to be highly desirable. If top hospitals systematically choose to hire clinicians as their leaders, those hospitals must believe they make effective leaders.
Second, in our study, hospital performance is based on outputs such as the number of outpatient and emergency patients and the number of hospitalisation days. Medical decisions about diagnosis and treatment forms 60%–80% of total hospital cost.48 Fee-for-service payments to physicians, which are common in Iran, may exacerbate the effect of physicians’ incentives for inducing demand.
Conclusion
Hospitals are complex social systems and managing them requires deep knowledge about their function. The medical-engagement literature suggests that having a medically trained leader enhances employee engagement which in turn influences performance.4 The theory of ‘expert leadership’49 suggests that core business experts, such as physicians and other clinicians, are more likely to understand the conditions in hospitals under which other expert-employees flourish, which raises worker job satisfaction.21
Although a physician usually inhabits the most senior position in Iranian hospitals (hospital director), the day-to-day running of hospital administration is delegated to a chief operating officer. It is this person that we focus on in our study. Among the chief operating officers, 41 of them (56.9%) are medically trained managers, the majority of whom are physicians (35). Six of the 41 are educated in nursing, midwifery and as anaesthetist technicians. The dependent variable in the analysis is the performance of hospitals, and the key independent variable is the nature of management expertise (medical/clinical or professional managers). Data Envelopment Analysis (DEA) is used to calculate a measure of the performance of the sampled hospitals.
Our results for Tehran show (in table 5 and figure 1) that hospital performance scores are higher where the chief operating officers are clinicians. We observe this systematic difference in performance across many types of hospitals, including among teaching and non-teaching hospitals. The study adds to growing evidence of a link between clinical leadership and better hospital performance.
References
Footnotes
Contributors Both authors have contributed equally to this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.