Article Text

Abstract
Background The COVID-19 pandemic impacted many aspects of normal operations in academic medicine. While effective leadership is always important, the intensity and urgency of COVID-19 challenged academic medicine leaders to find new ways to lead their institutions and manage their own experiences of the pandemic.
Methods Sixteen physician leaders from Michigan Medicine took part in semistructured interviews during April and May 2020. Participants were asked open-ended questions about the attributes and techniques that were important to effectively lead during a crisis. The authors analysed the interviews using thematic analysis.
Results Participants described three overarching themes of leadership during the COVID-19 pandemic: (1) bringing together a diverse team with clear, shared goals; (2) using a range of strategies to tend to their teams’—as well as their own—well-being; and (3) engaging in leadership reasoning as a way of learning from others and reflecting on their own actions to inform their future leadership practice.
Conclusion The results of this study reveal several salient themes of crisis leadership during the COVID-19 pandemic. The findings also highlight the role of leadership reasoning, a reflective practice employed by leaders to understand and improve their leadership skills. This finding presents leadership skill development as part of lifelong learning in medicine. Findings may be incorporated into best practices and preparations to inform future healthcare leaders.
- leadership assessment
- medical leadership
- clinical leadership
- learning
Data availability statement
No data are available.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Leaders are pivotal to an organisation’s success, and in times of crisis, a leader’s performance makes a profound impact.1 A crisis creates ambiguity for an organisation, necessitating urgent action to safeguard the organisation’s viability.2 Crises also unveil unique opportunities for leaders: followers look to them for direction,3 and followers’ organisational commitment and perception of a leader are enhanced.4 Beyond implications for both their followers and organisations, a leader’s response to a crisis reveals important lessons to inform future leadership.5
The COVID-19 pandemic is one of the most significant global health crises in recent history and requires strong physician leadership to navigate through it. There is a growing collection of literature on characteristics of physician leadership6–8; however, effective physician leadership during times of crisis is less well studied, and robust efforts should be made to understand the critical lessons leaders are learning during these times.5 To achieve this, we undertook this study to better understand key themes of physician crisis leadership during the COVID-19 response.
The pandemic creates an opportunity for leaders to reflect on their leadership and for learners to gain insights on how to effectively lead amid a global health crisis.9 The COVID-19 pandemic also poses a unique challenge for leadership education: in previous crises, including natural disasters or the September 11 terrorist attacks, medical trainees were actively involved in the responses. Yet, in an effort to socially distance and preserve personal protective equipment (PPE), medical students have been pulled from clinical rotations,10 and much of residency training was forced onto a digital platform to reduce clinical exposure and preserve an adequate workforce.11–13 While necessary, these efforts have challenged the education of our future healthcare leaders. Therefore, the need for innovative ways to educate trainees14 and impart physician leaders’ insights are as imperative as the need for strong leadership. The findings we share here emphasise the role of reflection on leadership performance as an element of lifelong learning, which we identify and describe as leadership reasoning.
Methods
Study design
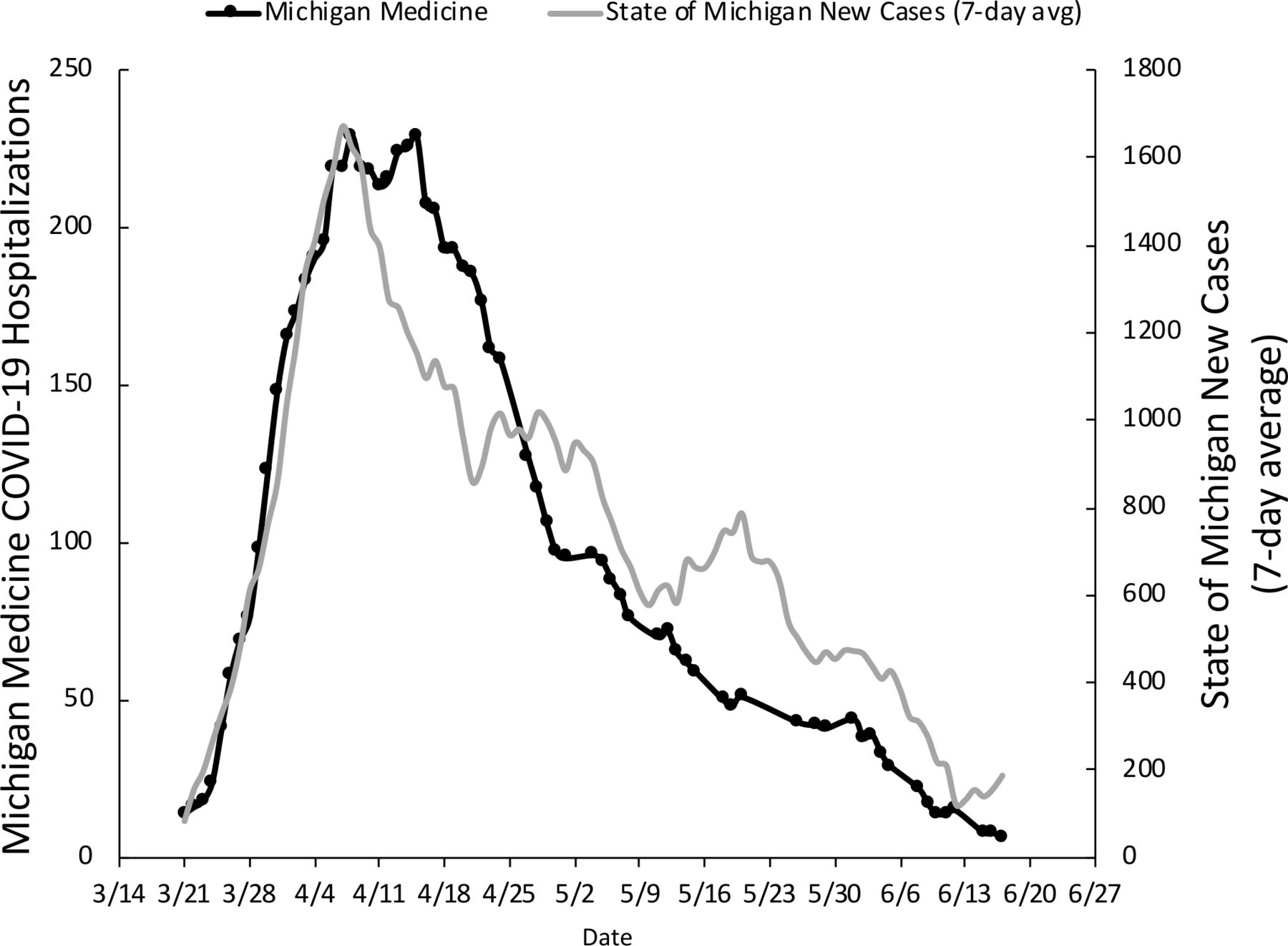
This investigation was conducted at Michigan Medicine, a tertiary academic medical centre. This institution received its first patient with COVID-19 in mid-March and was at peak capacity by mid-April (figure 1). In order to understand how institutional leaders carried out and reflected on their roles during the COVID-19 pandemic, we used thematic analysis to identify and analyse themes from qualitative, video-recorded interviews (n=16).
{kind=link}
Timeline of Michigan Medicine COVID-19 hospitalisations* and state of Michigan new COVID-19 cases† from 14 March 2020 to 27 June 2020. *COVID-19 update. https://www.uofmhealth.org/covid-19-update. published 2020. Accessed 14 June 2020. †Michigan data COVID-19 case by county. https://www.michigan.gov/coronavirus/0,9753,7-406-98163_98173---,00.html. Published 2020. Accessed 21 June 2020.
Study sample and recruitment
Using convenience sampling, we recruited three tiers of leaders: those who had a role that assigned them significant operational responsibility, those whose existing leadership role was augmented in the COVID-19 pandemic and those who were identified as emerging leaders during the research process. Established leaders were recruited from departments heavily involved in the COVID-19 response, the executive cabinet and other domains that responded to the pandemic by attending to educational and diversity, equity and inclusion concerns. As we began interviewing established leaders as well as those with augmented leadership roles, we used a snowball sampling strategy to recruit additional emerging leaders, asking participants to identify individuals who had taken on a new leadership role as the pandemic progressed. If an emerging leader’s name was identified more than once, they were asked to participate in an interview. Recruitment of established and augmented leaders was done via email with the support of a senior leader within the executive cabinet. Recruitment of emerging leaders was conducted by the study team directly. If we received no response, we sent one additional reminder email to elicit participation.
The final response rates to recruitment emails was 72% from our initial group of 18 established leaders and 75% from the four emerging leaders. The final sample included 16 leaders (12 men and 4 women). Of these, seven were established leaders, five had leadership roles that were augmented during the pandemic and three were emerging leaders (table 1). Although we had a significant gender imbalance, particularly at higher levels of seniority, this mirrors the gender breakdown of physician leadership within our organisation, as well as at academic medical centres nationally.15
Characteristics of 16 physician leaders at Michigan Medicine during the COVID-19 pandemic*
Data collection
Authors (TCS, DP, NT and KD) conducted 16 semistructured interviews lasting 30–60 min during April and May 2020. The interviews were video recorded using the Zoom platform in accordance with human subjects research regulations restricting face-to-face data collection during the COVID-19 pandemic. Multiple research team members were present at each interview; data collection and analysis were performed collectively. Additional team members include individuals with expertise in qualitative analysis (AV) and leadership theory (LG) who helped create the interview guide (online supplemental appendix 1). We developed the interview guide based on literature of leadership in crisis and used open-ended questions to elicit narrative responses. Participants consented to the analysis of their interviews as described below and also consented to the inclusion of interview snippets in a video about leadership during times of crisis to be made by the authors (TCS, DP, NT and KD). Participants received no incentives or compensation for their participation. Our institution’s institutional review board determined our study to be exempt research (HUM00180821).
Supplemental material
Deciding when to conclude qualitative data collection can be challenging.16 We conducted interviews until we heard no new insights arising during the interviews and were confident that our understanding of the common topics arising across respondents was deep enough for analysis. We arrived at this determination using a series of ongoing conversations about themes arising during the data collection process. We used this as a marker of data sufficiency in thematic analysis.17
Data analysis
Interviews were transcribed using Rev.com (San Francisco, California, USA) and inductively coded using thematic analysis techniques to generate and refine themes.18 19 First, three authors (TCS, NT and KD) independently coded three transcripts using the qualitative data analysis platform Dedoose V.8.0.35 (2018) (SocioCultural Research Consultants, Los Angeles, California). These authors compared codes and developed a codebook, using an iterative consensus-based process to establish agreement as they generated the remainder of the codes. Each interview transcript was coded by at least two research team members. Next, the authors began establishing the relationships between codes and grouped the codes into themes. Finally, the authors refined the themes as they produced the final analysis. Analysis was carried out under the guidance of senior author (AV), a trained qualitative researcher, and the findings are reported in line with the Standards for Reporting Qualitative Research.20
Results
Our thematic analysis allowed us to identify common experiences across this group of institutional leaders and generated three main themes (table 2): (1) leaders explained that COVID-19 brought together new team configurations with clear shared goals; (2) leaders used a range of strategies to tend to their teams’ and their own well-being; and (3) leaders reflected on their own performance during the crisis and how they learnt from other leaders.
Summary of leadership themes, subthemes and meanings during a crisis from qualitative interviews of leaders at Michigan Medicine during the COVID-19 pandemic
Theme 1: leveraging the unique circumstances of the crisis
Interviewees noted that the pandemic created unique circumstances for team collaboration. Often, effective leaders must create a vision for their team and build consensus around one common goal.21 22 However, in emergency situations, a common goal quickly emerges and a team’s focus shifts to patient care and crisis resolution.23 Many of our participants emphasised that the pandemic established a clear, time-sensitive mission of caring for patients that was almost self-evident. One interviewee compared the situation to a code scenario:
When you run a code, when a patient’s heart stops and an entire team of people run into a room, the easiest thing is that everyone in that room knows what their goal is and their goal is to somehow get that patient’s heart to start beating again. And so, in times of emergency, the cool part about it is that the purpose is clear. (Emerging leader)
The COVID-19 response also brought leaders together with new colleagues. Several participants appreciated the opportunity to work in multidisciplinary teams and learn from colleagues they did not normally interact with:
[Physicians] do things really differently, even managing the same disease process. And kind of acknowledging that and saying there’s not necessarily a right way to do this and we can learn from each other has also gone a long way. It’s been a good learning experience in sort of something that I’ve been trying to model. So, I think we’ve, we’ve learned from each other during this. It’s kind of been a nice, synergistic approach. (Emerging leader)
Participants reported a strong sense of a shared goal—to save as many patients as possible. Although there were many unknowns about caring for patients with COVID-19, participants expressed confidence that working in multidisciplinary teams would facilitate this.
Repeatedly, leaders distinguished between telling team members what to do and telling them how to do it. By reorienting to their team’s shared and obvious goal, leaders created greater engagement among team members, which could lead to a greater diversity of problem-solving approaches:
You can tell people what you want done, and then you’re kind of managing, ‘Are they accomplishing what it is?’ or you can tell people, ‘These are the things that we need to achieve,’ and you can get people working towards those achievements. And that gets you a much different level of engagement, much deeper level problem solving. Because if you’re back to the, ‘This is how to do it,’ all you’re going to get is what you can best think of yourself as how to do something. […] If you say, ‘These are the things we need to achieve, let’s achieve these,’ you’re going to get a lot better and diverse opinions and solutions on how to achieve those objectives. (Established leader)
Across leadership positions, our participants identified the overwhelming number of responsibilities created by the pandemic and explained that to succeed they must rely on their team. Engaging and empowering one’s team in collective problem solving has been identified as an effective tool of physician leadership.6 24 Our participants recognised that strong leadership required forgoing the common conception of a heroic crisis leader as a commander25; instead, they articulated high level goals and trusted their team members to act. In this way, leaders were able to harness the unique circumstances presented by COVID-19 to lead their teams effectively.
Theme 2: strategies for taking care of your team
Subtheme 1: emphasis on communication to build trust
Several participants described how the pandemic challenged their typical communication practices with their staff, who were encouraged to socially distance and overwhelmed by electronic communication.
Participants emphasised the power of being present and visible for their team. Being present, described as keeping their ‘boots on the ground’, enabled effective, closed-loop communication with staff. In addition to using physical presence to build credibility with their teams, leaders commonly spoke of the value of transparency:
I tried to be […] as transparent and free with information as I could be […] I think when people don't have a lot of information, your minds run and people gossip and everything feels maybe a lot worse than it is in that immediate moment. And so, as I had information, I really tried to pass it along in real time to empower people to feel like they had some sense of control and we would tackle the things that needed to be tackled and tried also not get ahead of ourselves. (Augmented leader)
Other leaders echoed this emphasis on transparency, extending it to include transparency around their own emotional experience of the crisis:
Being transparent and willing to admit strengths, weaknesses, fears, but also being willing to put yourself out there will go a long way. So I think it’s okay to say, ‘I’m really scared to be doing this right now and I don’t know what I'm going to do when I get home about keeping my family safe’. [It] probably is very meaningful to the sort of group of people around you who you’re leading, who were having the same concerns. And so hearing that we’re all going through this, but I’m also willing to go into that room and be with you and do that procedure. (Emerging leader)
A leader’s transparency increases followers’ perceived trust and their evaluations of leader effectiveness.26 In previous global health crises, healthcare leaders demonstrated transparency by acknowledging uncertainty rather than proclaiming confidence, which served to foster trust among their organisations.27 28 Our participants were not only transparent with information; they were vulnerable with their emotions. This runs counter to medical culture, which historically has had little tolerance for uncertainty29 30 and portrays physician leaders as directive and hierarchically oriented.31 In our sample, however, participants candidly shared their uncertainties surrounding confusing situations—and expressed their own fears about these uncertainties—to build trust and credibility with their teams.
Subtheme 2: tending to emotional and psychological well-being
In addition to using transparency, vulnerability and physical presence as a way to build trust with their teams, leaders deliberately acknowledged their staff members’ anxiety, stress and fear. One leader recognised the importance of responding to teams’ emotional needs because this restores the ‘human connection’ on the team and allows team members to release tension so that they can move forward with their work:
[The check-in] allows everyone to be heard, and also encourages participation because everyone is doing it, and it allows us to relate to each other as humans. And in this particular crisis, the human connection is so important because we’re not there physically next to each other. And [it] also allows people to be able to listen to the message and the issues that are coming next because we have allowed them to release a little bit of tension and a little bit of fear or whatever’s going on inside. (Augmented leader)
Interviewees described purposefully altering team dynamics in a variety of ways, such as ensuring their staff had explicit avenues to voice their concerns and felt both heard and appreciated:
We really, really did our best to both allow for a safe pipeline for communication and escalation of concerns and fears in a way that was psychologically very safe because I do think people really need to be heard. (Augmented leader)
Healthcare professionals experienced intense moral distress given the challenging circumstances that prevented them from providing the best patient care, including shortages of PPE and overwhelming patient volumes.32 Our participants anticipated that their staff would have concerns and created a sense of ‘interpersonal holding’33 by providing settings for staff members to share their concerns. As in prior research,34 our participants recognised that ignoring their team’s negative emotions would undermine the team’s ability to work together.
Just as leaders acknowledged the emotional toll the pandemic took on their teams, they also recognised their own moral distress, with some mentioning the effects on their team or family interactions. Participants described needing to reconcile their philosophies and values with necessary changes to respond to the pressing nature of the pandemic, and the rapidly changing decisions that leaders made were often contrary to their usual practices:
I realized I had just canceled a bunch of cancer surgeries, like functionally, and I’m a cancer surgeon. So then I got off the phone and I was like, don’t cry, don’t cry. (Augmented leader)
While making difficult decisions in a context of uncertainty added to their personal burden, it was often through these morally challenging decisions that leaders recognised key areas for growth.
Theme 3: using leadership reasoning
Scholars have noted that an important practice in developing leadership skills is to reflect, analyse and make sense of decisions made both by oneself and other leaders.35 One of our leaders described this as leadership reasoning, and others explained that applying the conclusions of this studied reflection is essential:
Thinking hard about those [leaders] that we look back on and say, ‘Wow, these were terrific leaders’. Taking a studied approach to that and saying, ‘What was it about those individuals that resonated so much with you?’ about their leadership and trying to pick up on what some of those elements are and trying to incorporate those elements into your own style. (Augmented leader)
Besides observing other leaders’ actions, our participants described continuous introspection throughout the pandemic:
One of the best skills […] is self-reflection. And that is looking back on how you think you’ve performed, […] to look back objectively and fairly, but with some level of critique and criticism, on either how you behaved in a circumstance and that either promoted success in that or did not, and to think about […]what you could have done differently or how you could have managed that differently. And then to […] distill that into either practices or principles that you would use going forward to be more effective. (Established leader)
Within a crisis, many participants acknowledged the distinct circumstance of seeing immediate outcomes from their decisions. Beyond expediting the consequences of their choices, the pandemic increased the number of decisions leaders were faced with. This created an enhanced opportunity for leaders to learn:
Well, the other nice thing is that things happen so quickly in a pandemic that the outcomes of the decisions [are] relatively quick. Usually if someone makes a bad decision, it’s apparent within 48 hours. […] You learned pretty quickly what works and what doesn’t. (Established leader)
Physician development involves being a lifelong learner36 and practising diagnostic reasoning to inform future practice.37 Just as morning rounds create an opportunity for clinical reasoning, participants took part in leadership reasoning. They viewed challenging situations as opportunities to learn from others and themselves and engaged in critical reflection to inform their future leadership. This focus on learning38 and critical reflection35 are skills of effective leaders, and despite the intensity and acuity of the crisis, our participants deliberately created space for these important practices.
Discussion
Researchers have reported that physician leaders perceive communication and interpersonal skills to be the most important leadership competencies.21 39 Our participants acknowledged the importance of communication for effective leadership and emphasised that the pandemic made high-quality communication a necessity. They described an ethos of transparency, which facilitated trust and tempered anxiety.
Participants supported their teams during the pandemic by actively acknowledging their staff’s psychological well-being and ensuring they felt heard. Healthcare professional burnout has already been on the rise in recent years,24 and the COVID-19 pandemic created a variety of new stressors including exposure risk, PPE shortages and social isolation.40 Additionally, studies have shown high levels of post-traumatic stress disorder41 and other psychological symptoms42 following previous global health crises, which linger long after the crises have passed. While there are limits to how well individual leaders can help their teams cope with problems of structural origin, our participants emphasised employing strategies to understand and mitigate their staff’s moral distress while simultaneously acknowledging and addressing their own emotions.
Previous research also indicates that moments of extreme stress provide powerful opportunities for leadership development.43 44 For our participants, the intensity of the COVID-19 pandemic allowed for more opportunities to engage in leadership reasoning. Just as frontline clinicians iteratively and collaboratively learnt how to care for COVID-19 patients,45 our participants learnt from other leaders, and themselves, throughout the crisis.
This study has a few limitations. First, the themes represented in this study were generated from interviews conducted at a single institution, and the findings may not be generalisable to other institutions’ leadership. Moreover, while interviewees spoke candidly about their experiences, they were speaking in their formal roles and with the knowledge that these interviews would be incorporated into a video montage to accompany this qualitative study. Additionally, we did not interview all the leaders involved in the COVID-19 response due to the large number of individuals in leadership at Michigan Medicine involved in the response. Consequently, the data do not represent the perspectives of all leadership positions and responsibilities in this time of crisis, although the leaders who participated do reflect three important types of leaders. Our study may have suffered from selection bias, as individuals who responded to the initial recruitment emails may have had more intense interest in leadership or leadership theory. Finally, the sample lacked diversity because most interviewees were male and white. While this racial and gender breakdown largely reflects the demographics of leadership at Michigan Medicine and in US academic medicine more generally,46 this lack of diversity precludes the insight on leadership during a crisis that leaders from other backgrounds may have. Indeed, because we used an inductive process to generate the themes in our analysis, one important implication of this lack of diversity is that the analysis reflects the perspectives of existing leaders, and our themes likely would have been different in a more diverse sample. Our study would have been unquestionably strengthened by including a more diverse composition of participants—and therefore opinions—and we encourage these efforts to begin upstream. In his viewpoint on realising diversity in academic medicine, Dr. John Carethers offers strategies to promote diversity in academic medicine through urging senior leaders to implement a diversity strategic plan and encouraging academic medical centres to embark on a fourth mission of the tripartite mission: diversity.47 We hope that these efforts will provide cohorts of leaders that are more representative of the organisations in which they serve and therefore will strengthen future studies on physician leadership.
Future inquiry comparing leadership during a crisis to leadership in ‘normal times’ is needed to understand the differences between these two states and if one has a greater effect on organisations and outcomes. Another area for additional research on leadership and COVID-19 will be exploring the postcrisis period to better understand whether leadership practices change in durable ways or revert to prepandemic patterns. Finally, as our study identified a psychological strain on leaders’ well-being throughout the pandemic, future work should compare the emotional burden on leaders to that of other non-leader health practitioners to understand how strain varies by leadership level.
Conclusion
Our study found that in response to the COVID-19 pandemic, physician leaders strove to empower and empathise with their teams and to be present, transparent and vulnerable in their interactions. Additionally, physician leaders and their teams faced great emotional burden because of COVID-19 but used the pandemic as an opportunity to engage in leadership reasoning in order to become more effective leaders.
Data availability statement
No data are available.
Acknowledgments
The authors wish to thank Carol R Bradford and Sanjay S Saint for their guidance and support in the inception and participant recruitment for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @T_Standiford
Contributors TCS and DP conceived the idea. LG and AV further developed study idea. TCS, DP, NT and KD recruited participants and performed data collection. TCS, NT and KD performed data interpretation and analysis. AV oversaw data analysis. TCS and AV wrote manuscript. DP, NT, KD and LG provided manuscript revisions. All authors have provided final approval for manuscript publication and agree to be accountable for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.