Article Text

Statistics from Altmetric.com
Integrated care systems are locality-based networks in England that bring together health and social care partners (including commissioners, providers and local authorities) to collectively plan services to meet the needs of the population. They are an example of collaborative governance, a governing arrangement that ‘brings public and private stakeholders together in collective forums with public agencies to engage in consensus orientated decision making’.1 One of the strengths of collaborative governance is the potential to include the perspectives and experiences of diverse stakeholders to generate creative, durable solutions to long-standing problems. In the case of integrated care systems, one of the key aims is to reduce the long-standing problem of fragmentation in care experienced by patients. However, decades of experiments with partnership working in health and social care have struggled with differences in culture, funding, timescales for decision making, and systems of accountability and regulation.
National policy identifies a key role for professional and clinical leaders in integrated care systems, building neighbourhood partnerships that span different services, and working with colleagues from different professions in designing clinical pathways across healthcare settings.2 Previous research suggests that medical leaders are well positioned to support collaborative governance. As hybrid medical managers, they are potential ‘boundary spanners’.3 Their membership of different professional communities gives them an understanding of different professional cultures, organisational politics and routine working practices; and helps with cross-boundary communication and engendering trust.4 They are also more likely than other professional groups to have ‘bridging’ relationships across organisations and professional groups, making them effective change agents.5
There is an urgent need to understand what makes collaboration between diverse stakeholders in publicly funded welfare services successful, and what medical leaders can do to support the collaborative process. Conceptual models can support leadership development and are valued by healthcare leaders.6 We use Ansell and Gash’s model of collaborative governance to distill learning from prior research.1 Based on a review of 137 case studies, across different policy sectors, including health, education, social welfare, international relations and natural resource management, the model sets out the critical variables that influence whether this mode of governance will produce successful collaboration. We begin by summarising the Ansell and Gash model of collaborative governance under the following headings: starting conditions, institutional design, facilitative leadership and the collaborative process (box 1). We then discuss the implications for medical leaders in integrated care systems.
The Ansell and Gash model of collaborative governance1
Starting conditions
The starting conditions influence the amount of trust in the system and whether this is a resource (high trust) or a liability (low trust) for collaboration.
Power and resource imbalances
Differences in the power and resources available to stakeholders leaves the system prone to disproportionate influence or manipulation by the stronger actors. In these circumstances, counter measures are required to represent less powerful interests. A key strategy is the use of facilitative leadership to include and empower less powerful actors.
Incentives to participate
Participation in collaborative governance is time-consuming and, therefore, depends, in part, on whether stakeholders believe the process will be meaningful. Stakeholders will decline to participate if they believe that their contribution is merely advisory or symbolic. An important incentive to participate in collaborative governance is recognition that stakeholders are interdependent. Even with a history of conflict and low trust, the acceptance of interdependence can lead stakeholders to participate and commit to meaningful collaboration.
History of cooperation and conflict
A history of cooperation between organisations and stakeholders furnishes collaborative governance with trust. In contrast, where there has been a history of conflict there is likely to be low levels of trust. Here, again facilitative leadership plays an important role in repairing relationships and building trust. This is often one of the most time-consuming aspects of collaborative governance.
Institutional design
Institutional design refers to the protocols and ground rules for collaboration, which are critical to the perceived legitimacy of the process. The most important design issue is inclusion—membership should be broadly inclusive of all stakeholders who are affected by decisions. Exclusion of stakeholders is one of the key reasons for failure. Other important design features are clear ground rules, process transparency and clearly defined roles, which are all important for procedural legitimacy and building trust.
Facilitative leadership
The role of leaders in collaborative governance is to promote and safeguard the process. Leaders are critical to bringing stakeholders together and guiding them through the process, especially difficult stages. Collaborative governance may involve multiple leaders, both formal and informal.
Leadership qualities depend on the individual context. In situations where there is relatively equal power relationships and strong incentives to participate, but low trust and high conflict, it is important for the leader to be viewed as an ‘honest broker’ who is ‘above the fray’. In these situations, someone from an external organisation may be employed as a neutral chair. Where there in unequal power between stakeholders, and uneven incentives to participate, an ‘organic leader’ may be more productive, that is, someone from one of the constituent organisations, who commands trust and respect. They will need to include and represent less powerful interests and persuade stakeholders to come to the table.
The process of collaborative governance
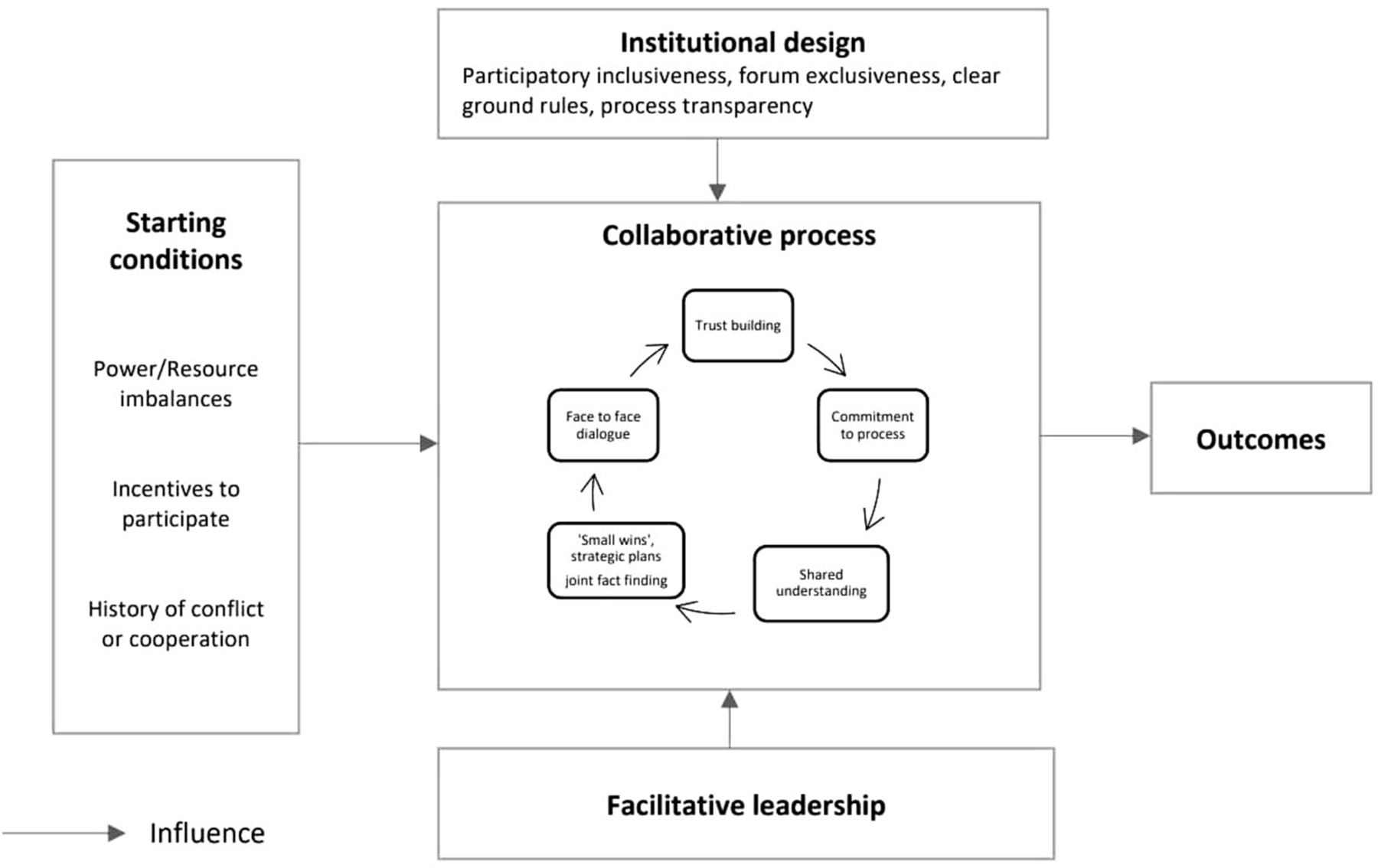
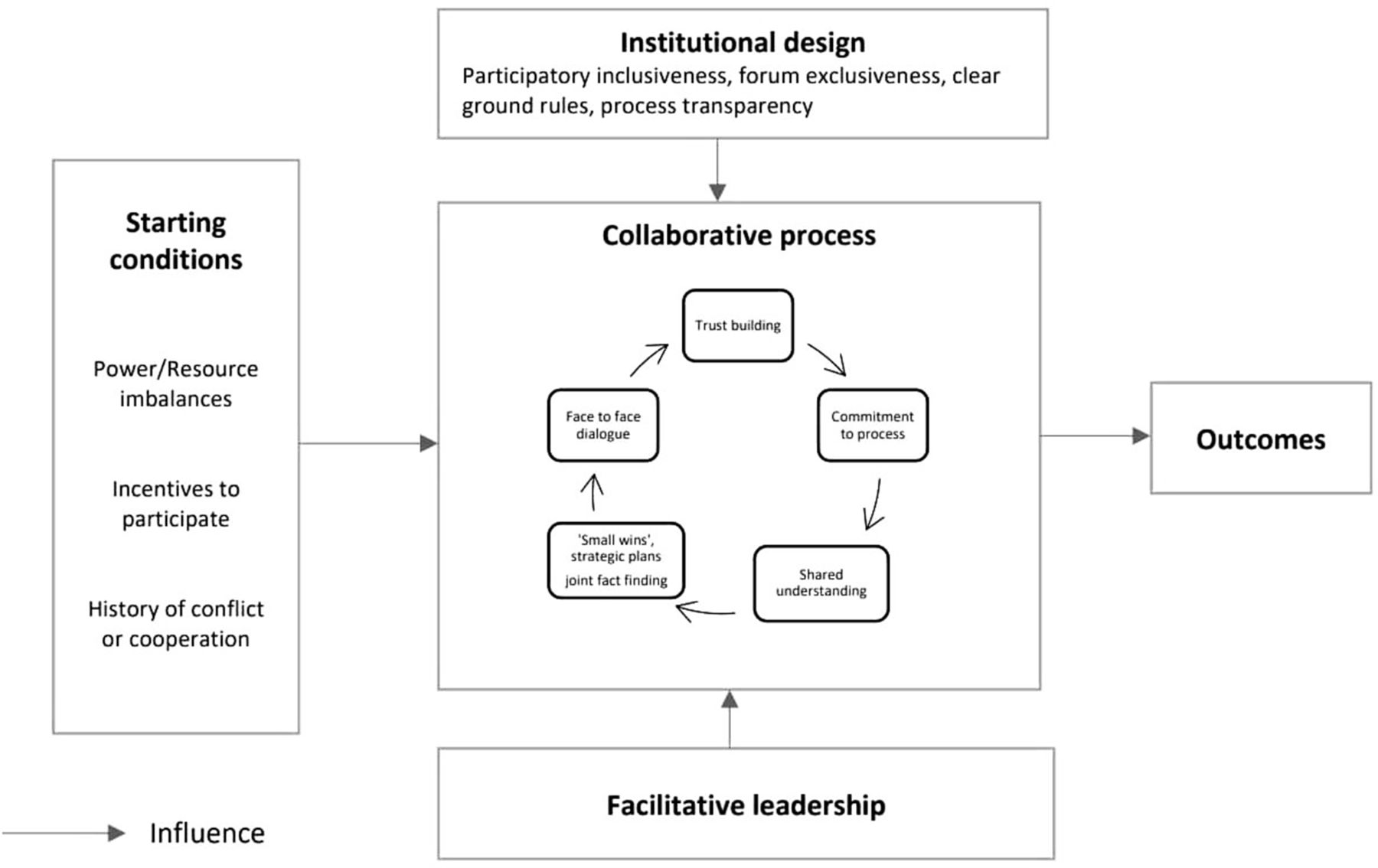
In figure 1, the process of collaborative governance is represented as a cycle to capture the way that successful collaboration can feed into a virtuous cycle of building trust, shared understanding and commitment to the process that leads to more successful collaboration.
Face-to-face dialogue
Face-to-face communication is helpful for exploring mutual gains and breaking down stereotypes about stakeholders.
Commitment to the process
Real commitment to the process of collaboration is a critical variable in explaining success or failure. For collaborative governance to work, stakeholders need to believe that good faith bargaining for mutual gains is a good way to achieve policy objectives. There also needs to be mutual appreciation. In other words, stakeholders need to trust that others understand and respect their perspectives and interests.
Small wins
Intermediate outcomes, such as strategic plans and joint fact finding, help to build experience of successful cooperation. Where there is a history of conflict and low trust ‘early wins’ are crucial to developing a virtuous cycle of successful cooperation, trust, increased commitment and further cooperation.
{kind=link}
Model of collaborative governance identifying key conditions for successful collaboration, from Ansell and Gash1.
Implications for medical leaders in integrated care systems
The Ansell and Gash model resonates with empirical findings from studies of regional health and care planning in England. For example, a recent study of medical directors found that they contributed important forms of ‘translation work’, ‘diplomatic work’ and ‘repair work’, to support planning and service development across professional and organisational boundaries.4 In the next section, we apply the evidence collated by Ansell and Gash in their model of collaborative governance to integrated care systems in the English NHS. We ask ‘what is the learning for medical leaders?’ ‘What challenges will they face?’ And ‘what skills will they need to develop to support and sustain the collaborative process?’
Starting conditions
Power and resource imbalances
The health and social care system in England is characterised by enduring power and resource imbalances, such as those that exist between primary and secondary care organisations, between health and social care, and between providers and patients.7 Therefore, a key role for medical leaders will be to include and empower less powerful actors. For example, by including and empowering less powerful organisations and patients, in developing safe, optimal cross-organisational pathways of care. Medical leaders may also need to reflect on their own position of power, stemming from their professional identity or organisational affiliation. In some cases, strategic inaction or absence may encourage participation and contribution from less powerful actors.
Incentives to participate
While for NHS organisations participation in integrated care systems is mandatory, it is not for all relevant partners, and for some key stakeholders there may be weak incentives to participate. The National Health Service (NHS) in England has a history of co-optive, rather than genuine, use of collaborative processes. For example, case studies of ‘codesign’ in controversial service reconfigurations have shown how decisions to close healthcare facilities had already been made, and other stakeholders viewed the forums as dishonest and manipulative.8 Medical leaders may, therefore, face challenges convincing stakeholders that it represents a meaningful attempt at collective decision making, rather than merely rhetoric or co-optation.
Integrated care systems require medical leaders to engage clinicians in service redesign. Medical leaders may face distrust from clinicians due to ‘initiative fatigue’ and previous experience of service change initiatives that have consumed large amounts of time and energy, only to be abandoned.4 Some clinicians may also fear the loss of the specialist service they provide. Recent research has highlighted the enduring emotional effects of organisational change.4 Feelings of loss and anger can last for many years and make staff reluctant to participate in further planning or service development.
Medical leaders will, therefore, need the skills and perseverance to engage clinical colleagues across healthcare. Clear articulation of the benefits to patient care is essential to engage clinicians. Medical leaders may also need to spend time listening and acknowledging the emotional effects of previous organisational change. Medical and clinical leaders will need to work closely together to encourage and support their colleagues. A failure to participate will mean decisions affecting their services and patients are made without them.
History of cooperation and conflict
While some systems in England have a firm foundation of successful joint working and trust between organisations and stakeholders on which to build, many have long histories of conflict and distrust, often the result of previous government policies, such as markets, mergers and reconfigurations of clinical services.4 In these situations, medical leaders will need to invest time in repairing relationships and rebuilding trust. Previous research has shown that rebuilding trust is often the most time-consuming aspect of collaborative governance. Ansell and Gash go so far to observe that:
If the prehistory is highly antagonistic, then policy makers should budget for effective remedial trust building. If they cannot justify the necessary time and cost then they should not embark on a collaborative strategy. 1
Institutional design
For successful collaboration, medical leaders will need to proactively include less well-represented stakeholders, promote ground rules and transparency, and share definitions of roles. Stakeholders entering a collaborative process will be concerned about the power of other stakeholders. Clear and consistent ground rules reassure stakeholders that the process will be fair and equitable, while transparency reassures stakeholders that the collaborative process is genuine and not a cover for ‘back room’ decisions.1
Facilitative leadership
Medical leaders will need to develop skills in promoting broad participation, encouraging participants to listen to each other, supporting productive group dynamics and helping stakeholders explore opportunities for mutual gain. Medical leaders can also play an important role in stimulating creativity by synthesising the knowledge of diverse participants to create new ideas.9
While medical leaders may fill the role of ‘organic leader’, known and trusted by constituent organisations, this may not extend to all settings and stakeholders. For example, local authorities, where accountability is based on democratic representation, may challenge the legitimacy of medical leaders. Community organisations, drawing from more social models of health and well-being, may also challenge the relevance of medical leaders.10 These contexts require medical leaders to understand the wider system in which health and care is delivered, appreciate the contribution and value of system partners, and acknowledge medical expertise is but one (although important) contribution to the complex system of health and care. Where there is high conflict and low trust, but relatively equal power relationships and strong incentives to participate, it may be helpful to have an external leader who is seen as neutral.
Leadership in integrated care systems will be complicated by ‘sedimented governance’.11 While integrated care systems are an example of collaborative governance, there are remnants of previous modes of governance, such as markets and hierarchy, leading to a complicated mix of governance mechanisms. Tax-funded systems, with ministerial accountability, can also expect to see the resurgence of hierarchy,12 a pattern that has been seen repeatedly over time in the NHS in England. In previous iterations of integrated care, the NHS hierarchy continued to exert pressure, even where formal structures had been dismantled.11 One way in which hierarchy continues to operate in collaborative networks is through metrics, which have the effect of capturing the focus of staff on the ground. Integrated care systems will be required to measure both activity and cost savings, which will make these objectives a priority for managers, competing with the priorities agreed on as part of the collaborative process.
Sedimented governance creates a challenge for medical leaders who may be seen as inheriting a regulation role while trying to build and maintain relationships. Research in complicated governance settings has found that one successful strategy for leaders is a ‘linking strategy’ based on understanding all three modes of governance (hierarchy, markets and collaborative networks) and translating between them as needed to make innovation happen, for example, investing time in meeting the needs of stakeholders in collaborative networks to feel included and appreciated, and making adaptations to meet the needs of hierarchical accountability.13
The collaborative process
In integrated care systems medical leaders can support the collaborative process by enabling face to face dialogue, building trust and helping to develop a shared understanding of the benefits to patients. For collaboration to be successful, there needs to be mutual appreciation of perspectives and interests. For some stakeholders this may require ‘a very significant psychological shift, particularly among those who regard their position in absolute terms’.1 Perhaps the key challenge faced by integrated care systems relates to commitment to the collaborative process. Participants need to believe that good faith bargaining for mutual gain is a good way to achieve policy objectives. This will require a significant change in mindset for NHS stakeholders used to responding to resource constraints by increasing ‘grip’.11 While national policy documents espouse the rhetoric of collaboration, they also suggest that the implications are not fully realised by policy authors. Integrated care systems continue to be seen as a way of implementing national NHS priorities,2 rather than as a way of deciding locally, collectively, what those priorities should be.
Conclusion
Based on empirical studies, the Ansell and Gash model identifies the critical variables for successful collaboration. It is a useful framework for medical leaders to understand the conditions required for integrated care systems to work, the key challenges they will face, and how they can support the development and sustainability of collaborative working. Integrated care systems require medical leaders to initiate and sustain cooperative working across multiple organisations, in most cases with little recognised authority. They will need to work beyond the specialty and organisational boundaries they are accustomed to and understand and appreciate the different actors in the system. Leadership development programmes should focus on the relational and diplomatic skills to repair relationships and rebuild trust; empower, persuade and negotiate; resolve concerns through dialogue; and engage patients and the public in decision making.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the reviewers for their helpful comments.
Footnotes
Twitter @dr_loreleijones
Contributors LJ, KA and PL contributed to the design. All authors contributed to the analysis, writing and final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KA, PL and AH are associated with the Faculty of Medical Leadership and Management which provides leadership development.
Provenance and peer review Not commissioned; externally peer reviewed.