Article Text

Abstract
Background COVID-19 screening protocols rapidly evolved as a result of changing Centers for Disease Control and Prevention (CDC) and California Department of Public Health (CDPH) recommendations. These protocols led to operational improvements at one large academic medical centre using change management methods explained in Kotter’s 8-stage change model.
Methods We reviewed all iterations of clinical process maps for identifying, isolating and assessing COVID-19 infections in paediatric and adult populations within one emergency department (ED) from 28 February 2020 to 5 April 2020. We incorporated CDC and CDPH criteria for the various roles of healthcare workers in ED patient assessment.
Results Using Kotter’s 8-stage change model, we outlined the chronological evolution of basic screening criteria, as well as how these were reviewed, modified and implemented during the onset and through the time of greatest uncertainty of COVID-19 in the USA. Our results demonstrate a successful creation, and subsequent execution, of rapidly changing protocols across a large workforce.
Conclusion We effectively applied a business change management framework to the hospital management response during a pandemic; we share these experiences and challenges to inform and guide future operational decision making during times of rapid change.
- communication
- management
- continuous improvement
Statistics from Altmetric.com
Introduction
The COVID-19 virus rapidly triggered a global health emergency alert from the WHO, with the first known case in the USA occurring in January 2020 and spreading to 46 countries by 27 February 2020.1 As cases spread within the USA, and globally, hospitals were forced to quickly implement protocols to screen, isolate and treat a surge of potentially COVID-19-infected patients. Changes in protocols required continuous awareness of transforming institutional infection control and local public health department recommendations, recursively communicating a new vision, bolstering morale and anchoring certain workflows as necessary components of ongoing change.2 These aspects presented unique challenges requiring a strategic approach in order to successfully adapt to the rapidly changing COVID-19 landscape.
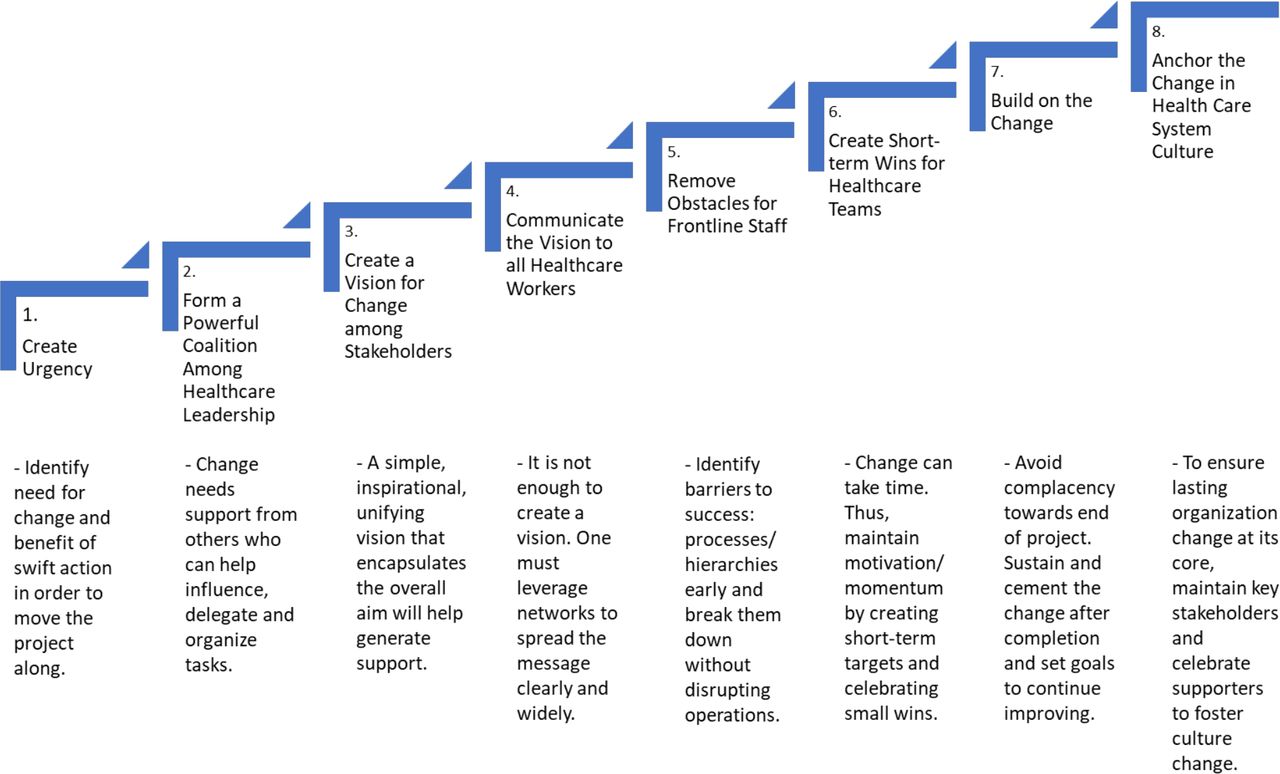
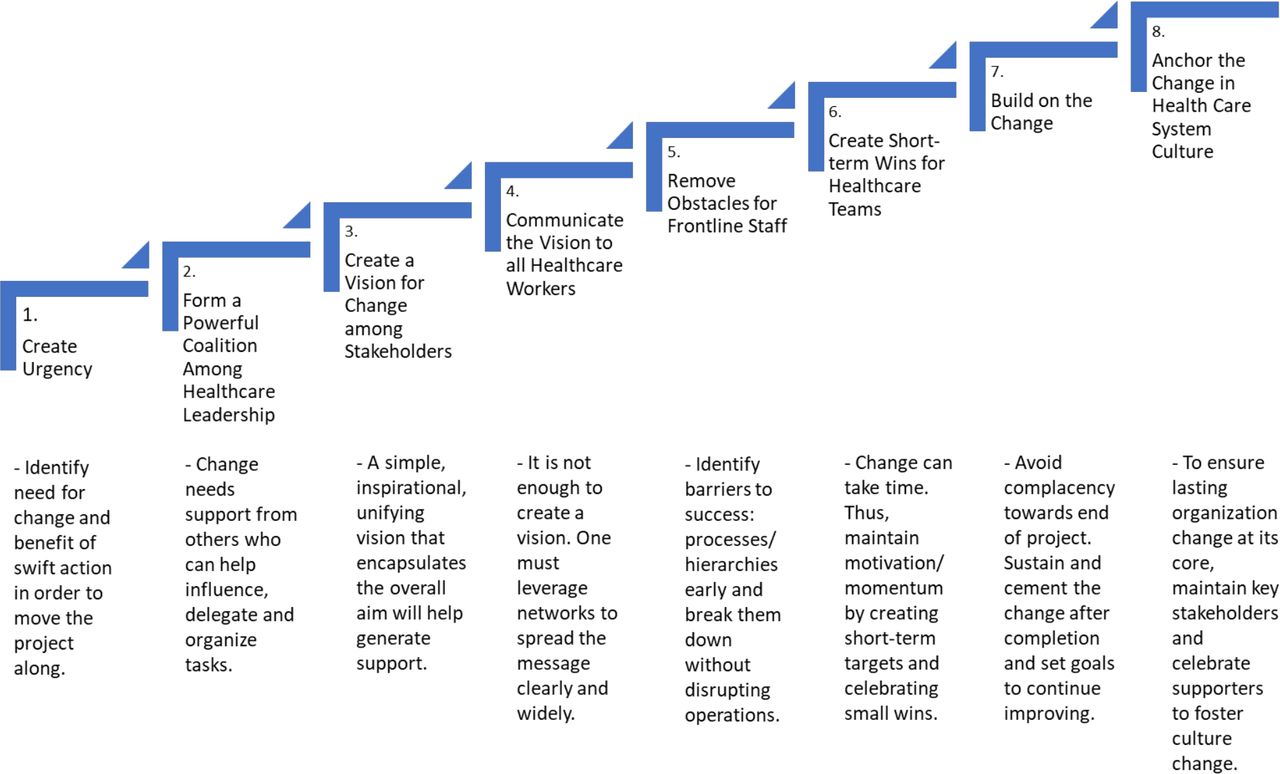
Approaches to effectively bring about change are often taught in business school, with the most frequently used being John Kotter’s industry-proven framework that outlines the eight-steps of the change process.3 Although seldom used for emergency department (ED) operations, our team recognised during the early implementation of these rapid changes that a change management framework should be guiding decision making. Although previous scholars applied other change management frameworks in healthcare settings, such as TeamSTEPPS and KINDER,4 5 we harnessed Kotter’s 8-stage change model (see figure 1) as our change management framework due to its broad applicability, proven success in other settings, and familiarity among our own operational leaders. Therefore, after evaluating all possible frameworks, we began purposefully using Kotter’s framework to focus decision making during the early stages of the pandemic This report describes the affordances of how using a corporate change model (ie, Kotter) during the pandemic supported us with managing acute healthcare challenges.
{kind=link}
Kotter’s 8-stage change model as a method of implementing impactful change in healthcare.
Methods
Setting
The ED at Stanford Health Care (SHC) is a tertiary care, level I trauma, academic department, with approximately 80 000 patients seen in 2019. We provide a retrospective report on the changes implemented across the combined staff of 90 attending physicians, 60 resident physicians, and approximately 200 clinical nurses.
SHC is a unique testing environment because on 3 March 2020, we were one of the first independent laboratories in the USA to implement an in-house-developed coronavirus PCR detection test within our clinical practice. As the pandemic progressed, Centers for Disease Control and Prevention (CDC) guidelines and California Department of Public Health (CDPH) recommendations changed more frequently. Concurrently, SHC guidelines were optimised to meet the need of frequently changing COVID-19 screening and care protocols. As volumes of patients under investigation (PUI) increased, triage workflows were changed, new pathways of transport were created, and new care areas were constructed for testing and discharging patients. Reporting requirements and responsibilities also changed as the pandemic unfolded.
Time frame
The first written departmental protocol regarding the triage and treatment of PUIs was disseminated on 24 January 2020. The next significant change occurred on 28 February 2020 as information regarding community spread in the USA became available. There were subsequently seven protocol changes between 28 February and 13 March (see table 1). The next change occurred on 5 April with continual change, although less frequently, as more knowledge of the virus and changing disease prevalence, testing recommendations and testing capacity occur. Although we have continued using Kottler’s framework to guide decision making through the multiple subsequent surges COVID-19 virus variants, this report focuses on the time period where the most rapid change occurred (ie, during the months of February through early April 2020).
Evolution of screening protocol and factors that influenced specific changes from 28 February 2020 to 5 May 2020
Results
Our results describe how our ED interpreted, accommodated and implemented COVID-19 CDC, CDPH and SHC guidelines to purposefully design and execute protocols. Table 1 shows the evolution of guidelines and protocols during COVID-19. Initially, CDC guidance was used in creating and updating SHC’s policy regarding COVID-19. Although with the development of SHC’s own in-house COVID-19 test, SHC’s institutional testing policy expanded beyond CDC and state testing recommendations. It is important to note that not all changes followed each and every one of Kotter’s stages to completion because of the rapidly evolving nature of the pandemic during these early stages; often, there was a need for multiple iterations of changes within a short period of time, usually days but sometimes hours.
Discussion
We did not initially embark on our pandemic management from the lens of change management because, at the time, we were unaware that the scale and frequency of changes could lend itself to such a framework. As the pandemic unfolded, however, our department grappled with approaches to quickly disseminate rapidly changing information, guidance and protocols to a large workforce of approximately 350 healthcare workers. Each subset of healthcare workers had their own management structure; therefore, the need to align nursing and physician leadership operating in parallel to share one coherent message was evident. The staffing and shift nature of the ED also meant that some staff members went up to 2 weeks without working and keeping abreast of changes to the clinical environment, and thus on return to the worksite, had to be easily and rapidly indoctrinated to new protocols.
Through multiple iterations of changing protocols, department leadership was able to learn best practices in implementing the changes. While small-scale changes can be implemented without much attention given to every stakeholder, the expanding changes of our COVID-19 protocols, each increasing in complexity over hours or days in the initial month, indeed benefited from a more robust framework. We recognised Kotter’s 8 steps in the midst of our changes as a suitable framework to describe the work already performed and guide future changes to ensure operational success and efficiency.
There initially was a suboptimal response from front-line staff to keep up with and adhere to the latest protocols. However, as cases spread throughout the USA in March, the urgency of the situation naturally evolved (stage 1), and the magnitude with which leadership spoke of patients and staff safety reached an all-time high. The Stanford COVID-19 command centre was developed early in the pandemic at the highest level of our enterprise (stage 2). As a result, the ED operations team formed a powerful coalition with the entire academic healthcare enterprise. This made information dissemination, delegation of essential tasks and many of the subsequent changes easier to implement (eg, an outdoor testing extension of the ED) thereby removing obstacles to change. Early in the change process, ED leadership communicated a vision for change through newsletters and townhalls, promoting the health and safety of our front-line staff and patients. The ED Chair promoted pride in being emergency healthcare workers in this time of crisis and heralded this as our specialty’s moment to shine; thereby creating a short-term win.
Then, we prospectively applied the change model in the form of community support and transparency to engender trust and appreciation during this crisis. We built on the change through an iterative process, repeating all or some of Kotter’s steps at each stage as needed, and anchored certain protocols through the electronic health records. Our process is not limited to the ED only. At SHC, primary care and specialty care clinics emulated our work as a leader for best practices in screening and testing, demonstrating that the Kotter framework can be generalised to across healthcare settings. While some existing literature outlines specific protocols regarding severity classification of COVID-19 infection, critical care management of diseased patients and presurgical planning,6 our description represents a more high level, systems-strategy approach to protocol selection, implementation and augmentation for current and future public health requiring rapid decision making.
Limitations
The approach outlined in this paper represents what was done at a single institution. We did, however, provide an alternative lens using an framework from outside of healthcare to evaluate a formal process for implementing changes related to the COVID-19 pandemic. We were fortunate to have early development of our own institutional assay as well as a team of individuals facile with Kotter’s change management framework and recognise that this afforded us opportunities that would likely not have been available to other EDs. Finally, our work is descriptive and does not provide quantitative data to support the effectiveness of our decisions, but future studies could be performed to further evaluate the consequences of this approach from an epidemiological, patient safety and financial perspective.
Conclusion
The COVID-19 pandemic forced our ED to be malleable and using a framework to disseminate rapidly changing guidance regarding the care of potential COVID-19 infected patients helped guide system-level decision making. The initial actions and subsequent formal adoption of Kotter’s 8 stages of change effectively allowed our clinical operations team to effectively keep our physicians and nurses abreast of the most recent care protocols, which was evidenced by feedback received in subsequent town halls. We maintained uniform, evidence-based care for our patients in a high-stress environment, and ensured a safe setting and a confident, informed workforce while addressing this global pandemic. While the rapid iterative changes described in this paper were implemented in an ED, the change process described can be applied to any healthcare facility where new information results in rapidly changing policies.
Ethics statements
Patient consent for publication
Footnotes
Contributors All listed authors were contributors to this submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.