Article Text

Abstract
New technologies including digital health and robotics are driving the evolution of healthcare. At the same time, healthcare systems are transitioning from a multiprofessional model approach of healthcare delivery to an interprofessional model. The concurrence of these two trends may represent an opportunity for leaders in healthcare because both require renegotiation of the complex division of work and enhanced interdependency. This review examines how the introduction of new technologies alters the role boundaries of occupations and interdependencies among health occupations. Based on a scoping review of ethnographic studies of technology implementation in a variety of contexts (from primary care to operating room) and of diverse technologies (from health informatics systems to robotics), we develop the concept of role reconfiguration to capture simultaneous adjustments of multiple, interdependent roles during technological change. Ethnographic and qualitative studies provide rich, detailed accounts of what people actually do and how their work and role is changed (or not) when a new technology arrives. Through a synthesis of these studies, we develop a typology of four types of role reconfiguration: negotiation, clarification, enlargement and restriction. We discuss leadership challenges in managing role reconfiguration and formulate four leadership priorities. We suggest that leaders: redesign roles proactively, paying attention to interdependencies; offer opportunities for collective learning about new technologies; ensure that knowledge of new technologies is distributed across roles and prepare to address resistance.
- clinical leadership
- healthcare planning
- health policy
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
New technologies including digital health and robotics are among the factors driving the evolution of healthcare. The integration of digital health and robotics into health services is expected to lead to improvements in medical diagnosis, prevention and treatment of diseases, surgical interventions and long-term care. Digital health is expected to promote effective and automated work management processes. Innovations in the field of robotics offer a wide range of applications in healthcare with the potential to make medical procedures safer and more cost effective.1 The promise of vast new efficiencies afforded by health technologies has attracted interest from both health systems, overwhelmed by the increasing complexity and costs of care,2 and technology companies worldwide. As a result, the rapid adoption of digital health and robotic technologies is predicted.3
At the same time, healthcare systems are attempting to transition from a multiprofessional approach to healthcare delivery to an interprofessional approach. This shift is intended to refocus the organisation and management of work away from each professional group and towards interprofessional teams. The interprofessional model aims to improve team dynamics and processes, thus enhancing collaboration among professional groups by developing shared goals, clear team roles and integrated work practices.4 This approach is promoted as a means of better managing the ever-growing complexity of delivering healthcare and improving its effectiveness.5–7
The concurrence of these two trends may represent an opportunity for leaders because both challenges require renegotiating the complex division of work in healthcare and increasing collaboration among professional groups. We draw on ethnographic studies of technological change in healthcare settings to understand the implications of technological change for work roles and collaboration. New technologies create new tasks, automate or eliminate established tasks and shift tasks across professional groups, requiring that workers develop new skills and knowledge, accept changes to their job role and work with others in new ways. These disruptions usually create direct effects for two or more professional groups and create indirect effects for adjacent professional groups. Overall technological change generates role-reconfiguration adjustments in boundaries8 across multiple, interdependent roles. We synthesise findings about role reconfigurations from social sciences and health services. These findings suggest how leaders can trace and anticipate role reconfigurations in a way that supports technological change in healthcare. Studies of technological change offer valuable insights about the intended and unintended consequences of integrating a new technology8 in interprofessional healthcare teams.
Methods
Design
We conducted a scoping review to systematically synthesise the findings of ethnographic studies of the implications of technological change for work and roles in healthcare. We selected topically relevant studies that employed ethnographic methods. Ethnographic studies provide detailed empirical observations about the work done, including collaboration and communication patterns, the interpretations and meanings of the work (from the workers’ perspective) and the use of technologies (new and old). Given this, ethnographic studies are most appropriate for understanding how the integration of new technologies changes what workers do, how they do it and with whom they collaborate. While discourse studies of new technologies, and adoption, and interviews and surveys to change adoption are extremely valuable, they do not track and examine change at the level of daily work and interactions. This is in part because of the level and unit of analysis employed and also because we know that formal definitions of roles and verbal accounts of roles, detached from their doing, do not correspond accurately with what people do at work.9 Overall, we focused our review on relevant papers most likely to facilitate the development of new understanding of how technology changes work, roles and collaboration.
Criteria for including studies
The inclusion and exclusion criteria are shown in table 1. We identified ethnographic studies investigating the introduction of new technologies across different healthcare settings (from primary care to operating room) and of diverse technologies with interdependent users (from health informatics systems to robotics). We excluded studies that treated technology as a type of knowledge or as soft technologies such as new skills.
Inclusion and exclusion criteria
Search strategy
Initial searches in peer-reviewed health science journals were conducted in June 2019 (figure 1). The search was limited to a 2-year period (2017–2019) because of the growing interest in health technologies and studies related to this thematic. The goal was to identify the most recent publications in high-ranking, peer-reviewed health science journals. The full list of search terms was built iteratively and informed by the results in each database (see online supplemental file 1).
Supplemental material

PRISMA flowchart of identification and inclusion of studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Organisational journals
The references of retrieved articles indicated organisation journals as a useful source for ethnographies of work. A manual search of organisation journals was undertaken (see online supplemental file 2). No date restrictions were applied to organisation journals because there were few studies related to our search terms published between 2017 and 2019.
Supplemental material
Bidirectional citation chasing
We used a bidirectional citation chasing approach to generate a full list of qualitative references describing the implications of technological change for work and roles in healthcare (see online supplemental file 3). The initial references in this instance were the five papers sourced in the database search8 10–13 and the seven papers from the manual search.14–20 Through the citation chasing process, 12 additional papers were identified.21–32
Supplemental material
Data analysis
We used Nvivo V.11 software to organise and support our analysis. Through open coding and constant comparison, we inductively developed the role-reconfiguration concepts presented below. The movement between the codes and the eventual concepts was iterative, meaning that we wrote, developed schematics and worked with the codes in numerous ways until we identified and articulated patterns across the literature. Full details of data extraction can be seen in tables 2 and 3.
Data extraction table: characteristics of included studies
Data extraction table: themes from analysis
Results
Role reconfiguration
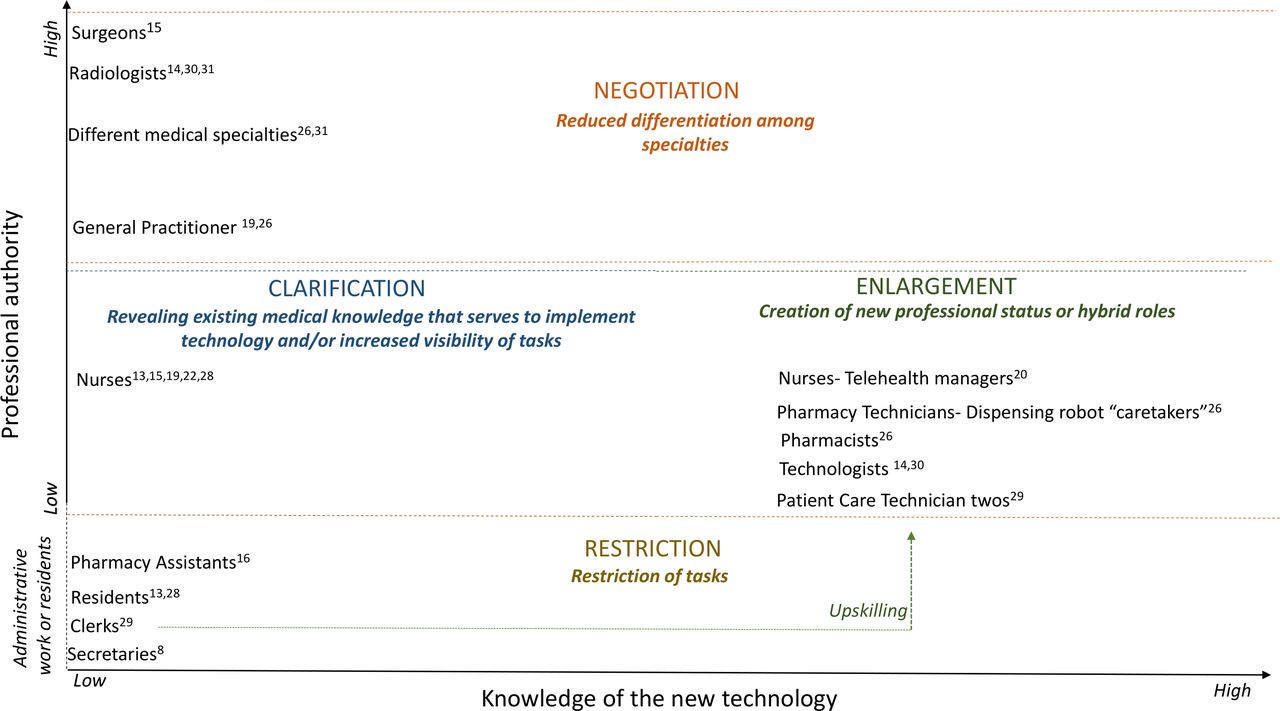
There is consensus across the studies that technologies serve as an occasion for role reconfiguration. The implementation of new technologies depends on changes in the tasks, interactions and knowledge of professional groups. Our analysis reveals four themes pertaining to the reconfiguration of roles—negotiation, clarification, enlargement and restriction—which relate to authority and knowledge structures as depicted in figure 2. In the context of professions, authority is the right to issue commands related to a set of tasks. Members of a profession claim authority when their profession has the regulatory right or most appropriate expertise to address a social problem.33 The y-axis shows professions distributed across this range of authority, highlighting medical dominance—physicians’ authority over other professions—as the traditional organising principle in healthcare delivery. The x-axis refers to knowledge about how to apply and monitor them in healthcare settings.
{kind=link}
{kind=link}
Model outlining the four types of role reconfiguration.
Overall, when a new technology is implemented, roles tend to be altered according to their degree of professional authority and their knowledge of the new technology. Roles may be enlarged or restricted, clarified or negotiated. Those with high degree of authority—physicians—have the privilege of negotiating their roles in ways that may reduce differentiation among medical specialties affected by the new technology. Nurses and allied professions tend to have their roles clarified and enlarged by the new technologies. Workers out of the scope of clinical practice, but who offer administrative support to clinical work (ie, secretaries, clerks) or support medical practice as part of a learning process (ie, residents), often have their roles restricted.
When a new technology is introduced, knowledge of this technology—knowledge about how to apply, monitor, adjust and evaluate it—allows those who develop this knowledge to have a better control over their work. Often this leads to an expansion of their role, creating new dynamics with those working around them who do not have knowledge of the technology. The knowledge of the new technology seems to be the main force that triggers enlargement of roles. We describe each form of role reconfiguration1 and highlight leadership priorities during technological change to ensure the successful integration of digital health and robotics into interprofessional health services.
Negotiating roles
Physicians, because of their professional authority, are able to interfere in the successful implementation of new technologies. This occurs when physicians continue to work as usual around the new technology rather than altering their work practices and clinical interactions with other team members, in relation to the new technology. A comparative case analysis of the implementation of a new cardiac technology across 16 American hospitals found that successful implementation occurred when the healthcare teams reconsidered the way they worked, shifting tasks and changing their coordination practices.16 Because of their professional authority, physicians can be central in leading and directing such changes in teams. When physicians do not integrate new technologies into their work routines, those working around them are less likely or able to do so.
Given this, the technological implementation process relies on physicians (ie, surgeons, radiologists, general practitioners and other medical specialists) to renegotiate the boundaries of their roles within their team.19 28 A central part of this negotiation is accepting that there is a new distribution of expertise or ‘who knows what’ on the team. Except in the case of robotic surgery, technologies are often known and controlled by technicians or members on the team other than physicians. This means that physicians have to rely on and coordinate with members of the team in a new way that often alters the distribution of authority and thus the power differential among members of the team.28 The introduction of new technologies requires that physicians develop expertise about how to work with the new technology or accept the value of this expertise in others.
Barley31 and Black et al 15 discuss how CT scans made the expertise of radiologists and technicians inseparable. The expertise needed to conduct a CT scan and the expertise needed to interpret the images were no longer clearly defined and separable, as they were with X-ray technology.15 31 Radiologists had to change the way they worked with technicians, becoming more interdependent and collaborative with technicians, thus shifting the boundaries of their role and the technician role.32 Similarly, a new technology for cardiac surgery increased communication and interdependence across professions, changing the team member’s task and blurring the former hierarchy of team roles.16 By changing the distribution of expertise and tasks, technological change shifts power relations among team members.20 Such shifts often require physicians to relinquish the traditional notion that they are the most knowledgeable member of the team, accepting that knowledge of how to use new technologies and interpret their outputs is integral to medical care and sharing authority with those who have such expertise.
Clarifying roles
Nurses and allied health professionals often possess unnoticed medical knowledge. These practitioners learn by working closely with physicians in daily clinical practice, developing knowledge and skills that are not formally recognised by the organisation. The introduction of new technologies often reveals and clarifies the actual tasks nurses perform and the related medical skills and knowledge required to perform these tasks.26 In doing so, the technology also reveals overlaps in task, skills and knowledge among members of the team. For example, the introduction of telemedicine enabled managers to recognise the knowledge that nurses had in handling specific drugs—a task previously reserved only for physicians.20 The introduction of robots into operating theatres has revealed the latent knowledge and skills of nurses who are now responsible for the direct physical manipulation of instruments through the trocars inside the body of the patient. They did not perform these tasks prior to the introduction of the robots but had the knowledge of how to do it because they had observed and assisted surgeons doing it for years.29
Often the nurses’ unacknowledged knowledge and skills are revealed by the spatial and temporal separations of the work of nurses and physicians created by new technologies. As nurses work asynchronously and at a distance from physicians, it is possible to observe their skills and knowledge in a new way. Pelikan et al 23 show how a tele-operated surgical robot reconfigured teamwork. As the surgeon moved from the patient’s side, registered nurses took their place, supporting the surgeon by controlling the suction machine and changing the instruments. These nurses already had the skills to act as first assistants, mediating the interaction between nurses and surgeons during the surgery.
The recognition of the actual tasks, skills and knowledge of nurses is made possible by the introduction of new technologies. At the same time, the smooth implementation of these technologies is made possible because nurses have this unacknowledged experience and related skills and knowledge. One of the important implications of role clarification is that it leads to role enlargement (discussed next). However, most studies show that the enlargement of nursing roles through additional tasks and responsibilities is not recognised by management and their organisations. Role clarification, without official enlargement of roles, enables minor changes in the control of medical techniques (ie, nurses controlling the suction machine, manipulating surgical trocars, triaging patients) but does not create changes in professional authority. When this happens, new technologies solidify the subordinate position of nurses. Despite clarifying their increased skills, knowledge and responsibilities, nurses are simply asked to do more for the same working conditions and employment relationships.27 We suggest that this is highly problematic from a number of perspectives and discuss how leaders can address this issue below.
Enlarging roles
Professions that are able to enlarge their roles during technological change have some degree of professional authority (ie, nurses, pharmacists) and develop knowledge and skills related to the use of the new technology. Hence, they have the opportunity to negotiate control over this new technology, and through this they enlarge their role or develop new hybrid roles. Segar et al 21 describe how technological change provided a career change opportunity for nurses. Working with telehealth allowed nurses to move from ‘hands on’ nursing to telehealth managing. This enlarged role was considered by the nurses to be a less physically and emotionally demanding activity than nursing work. Barrett et al 17 found that introduction of a dispensing robot in pharmaceutical work enabled enlargement of the technician’s role in dispensing medications and provided technicians a more prestigious professional identity. Similarly, the dispensing robot provided pharmacists an enlargement of their role in patient-centred work and research, reasserting their privileged position in the pharmacy hierarchy. This was possible because the dispensing robot allowed pharmacists to maintain control of the dispensary at a distance and freed up their time to engage in other specific and more complex activities.
In these examples, nurses and technicians proactively became expert users of the technology, and in doing so they moved into new roles as telehealth managers21 or caretakers of the robot.17 Bergey et al 30 describe how unit clerks experienced an enlargement of their roles following the implementation of a health information system. A new hybrid role was created combining basic patient-centred care responsibilities (ie, answering unit call lights) with user knowledge of a new health information technology.
Restricted roles
Healthcare roles with limited authority (eg, medical secretaries, clerks and in some cases medical residents) are often ‘restricted’ during the implementation of new technologies. These roles may be eliminated because of the automation of all tasks or deskilled because challenging tasks are automated or assigned to other roles. In the latter case, technological features allow those with superior authority to work with restricted help from assistants or residents. Opportunities to develop knowledge about the new technologies are often foreclosed to people in these roles. They may learn these new technologies informally on their own initiative.14
Examples of roles being restricted are numerous. The implementation of a pharmaceutical-dispensing robot limited the autonomous work of pharmacy assistants.17 Before implementation of the dispensing robot, assistants could work with little supervision from technicians or pharmacists. However, some robotic features reinforced the hierarchy of pharmaceutical work and the well-established distinctions between assistants and the other two occupational groups (technicians and pharmacists). Similarly, the introduction of a health information technology system reduced various tasks that clerks previously addressed, such as copying and entering orders. Unit clerks thus had less job security.30 Medical secretaries lost their jobs after implementation of a speech recogniser device, as their transcription services (their primary task) were no longer needed and the hospital used this restriction as an opportunity to pay for the new technology.8
When new technologies enlarge roles by shifting tasks down the chain of medical expertise, those in training—such as residents—may find their roles restricted. For example, the adoption of robotic-assisted surgery can trigger a shift of simpler tasks from surgeons to scrub nurses, limiting the opportunities the resident has to participate in their mentor’s work.14 29 The introduction of a robot in the operating room increased the physical distance between surgeon and other professions, a change that limited learning and teaching opportunities for residents.14 29 Residents, who used to assist surgeons, have their role restricted in the surgical team, spending the majority of time watching the surgeon operate the robot, rather than participating.14
Leadership priorities during periods of technological change
Leaders appreciate the importance of actively managed technological change, guiding activities towards organisational goals and in alignment with organisational values.34 A key task for healthcare leaders is to recognise how roles may be reconfigured in the midst of technological change and to anticipate challenges inherent in role reconfigurations. Role negotiation, clarification, enlargement and restriction show how interdependent work around new technologies is restructured, often disrupting the established division of labour, including embedded knowledge and authority hierarchies. We suggest four ways that leaders can facilitate constructive role reconfiguration during periods of technological change.
Proactively redesign roles and interdependencies
Technological change requires that managers evaluate jobs and their design. In such evaluations, a task analysis of jobs prior to and following the implementation of a new technology can help assess the need for a redistribution of tasks across roles. This allows managers to identify the need for each form of role reconfiguration and to facilitate it.
When technology clarifies roles, leaders face the decision of whether to formally recognise the formerly unrecognised skills, knowledge and tasks. This acknowledgement could take multiple forms including new job categories, titles and rewards. In situations where this acknowledgement is difficult or requires time, leaders may consider intermediate measures such as verbal and symbolic recognition. Failure to recognise gaps between actual and recognised work may lead to decreased motivation and cynicism.13 Another potential challenge, not explored in the literature, is the implications of such revelations for physicians. How do physicians experience passing off tasks, even mundane ones, to nurses? What is lost in the physician–client relationship?
The elimination of roles and deskilling of roles due to technological change is an old story.35 However, the process through which roles are restricted and the unanticipated side effects are important to consider. In the case of automating the work of assistants and secretaries, healthcare organisations are at risk of losing long-term employees with significant organisational knowledge related to operating processes, legacy technologies and idiosyncratic people.36 This can be disruptive to operations. This is in addition to the well-known negative reverberations of lay-offs.37 Further, the restricting of some roles often means that other roles are being enlarged. The simultaneous enlargement of related roles should be recognised, and some amount of time and support is necessary for new tasks to be absorbed into other roles.
Offer collective opportunities to learn about the new technology
The studies we reviewed highlight the importance of collective learning as key to determining whether a technology takes hold or not.15 16 38 This is important because new technologies tend to require improvements in interdependency and closer work between professions.10 24 Moreover, for many technologies, new technical and social knowledge must be transferred to enable use. This transfer of knowledge, that is part of the role reconfiguration, is not a single act but discrete steps of enrolment, preparation, trial and reflection across professions.16 Collective opportunities to learn about the technology can enable health professionals to recombine their knowledge in a meaningful way during technological change13 18 20 and allow professions to move to enlarge their roles. For those for whom a role enlargement is expected, the leadership challenge is to promote learning opportunities that open up possibilities for upskilled jobs in healthcare that might ultimately improve the quality of healthcare services.
Distribute expertise of the new technology
To help healthcare teams realise the benefits of a new technology, leaders can promote strategies to sustain the development of a balance of expertise across groups. Such a balance of expertise of the new technology should be a leadership priority, as it allows productive interactions between professions and sustains a collaborative pattern instead of fear and anxiety.15 Knowledge transfer and support from those with expertise in the new technology can facilitate its successful integration into daily work.11 If leaders do not encourage a balance of expertise, some professionals who know more than others about how to use the technology are likely to dominate the use of it, accumulating more knowledge of the new technology and reinforcing a pattern of professional dominance instead of collaboration.15 31 Furthermore, we argue that a balance of expertise could favour the observability attribute required for the diffusion of innovation. The observability is defined by Rogers as the ‘degree to which the results of an innovation are visible to others’. It has been positively correlated with the rate of acceptance of a new technology.39 We believe that a shared understanding of the new technology and its potential results and benefits could motivate the adoption of an innovation across professional groups.
Expect and address resistance
The introduction of new technologies can open space for more interdependent work; however, this is more likely to happen when some professionals renegotiate their roles on the team, yielding their authority and adjusting their practice to support technological change. Leaders may want to include health professionals in the design and the implementation phases in order to design the functions of technologies and negotiate their roles.8 It is particularly important to plan how different professionals can recombine their work during technological change.40 ,11 Moreover, by allowing participation of professionals in the design and implementation phases, leaders have the opportunity to discuss the benefits of new technology and negotiate changes in their expertise-based authority.
Professionals can be resistant to implement and have a negative outlook towards a new technology due to technology anxiety and fear that it can change the present work practices,22 41 42 undermine professional roles21 and restrict their roles. Overall, leaders have to encourage all team members to articulate their concerns and be active in the change process.16 An open attitude from leadership is central to breaking down barriers to collaboration and can encourage the establishment of new ways of working together around the new technology.10
The literature also suggests that leaders handpick a team of professionals dedicated to piloting the technological change.13 16 Randel et al.13 describe how a team selected by managers (to undertake technological training abroad) felt privileged and motivated to work to overcome the challenges of robot-assisted surgery, despite changes in their workload. Leadership can also ensure that professionals have more time in their working day to spend on the new technology.12
Conclusion
This review shows the role-reconfiguration effects of technological change. We identify four types of role reconfiguration: negotiation, clarification, enlargement or restriction. Our findings emphasise the importance of leadership during periods of technology change. Leaders should anticipate and acknowledge role reconfiguration. Leaders may facilitate the enlargement or restriction of roles, the latter being a difficult challenge. The leader may foster the negotiation of roles, particularly among medical specialists. The negotiation roles need to be facilitated among physicians and other members of the healthcare team (nurses, pharmacists, technologist, technicians, others), clarifying the relationships between professional autonomy and knowledge of the new technology.
Leadership may strengthen both trends—new technology changes and interprofessional work—by facilitating the development of a shared understanding of each team member’s role and their interdependencies. The possible tensions that can emerge between them may be useful to promoting collective opportunities to learn about new technology and encouraging a balance of technological expertise among team members.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HA made substantial contributions to all aspects of the study and manuscript, including: the design and execution of the study; the analysis and interpretation of the data; theorising the findings and drafting of the paper. RH made substantial contributions to the interpretation of the analysis, theorising the findings and drafting of the paper. MP made substantial contributions to revising the manuscript. HA, RH and MP have given final approval of the version to be published. Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content. HA, RH and MP have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Funding for this study was provided by the Coordination for the Improvement of Higher Education Personnel, Brazil, for funding this research (National Thesis Award 88887.357373/2019–00).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
↵The patterns that we identify are roughly consistent with the polarisation effects of technologies on skill demand and wages identified by economists. (Autor, D. H., Levy, F., & Murnane, R. J. (2003). The skill content of recent technological change: An empirical exploration. The Quarterly Journal of Economics, 118(4), 1279-1333; and Autor, D. H., Katz, L. F., & Kearney, M.S. (2006). The polarization of the US labor market. The American Economic Review, 96(2), 189–194). However, our analysis reveals the mechanisms and dynamics involved in technology implementation at the level of role systems rather than individual jobs in isolation. This lens indicates that there are ways to implement such technologies to complement all roles in the system rather than simply upskilling and deskilling. This requires engaged and thoughtful leadership.