Article Text

Abstract
Power and leadership are intimately related. While physician leadership is widely discussed in healthcare, power has received less attention. Formal organisational leadership by physicians is increasingly common even though the evidence for the effectiveness of physician leadership is still evolving. There is an expectation of leadership by all physicians for resource stewardship. The impact of power on interprofessional education and practice needs further study. Power also shapes the profession’s attempts to address physician and learner well-being with its implications for patient care. Unfortunately, the profession is not exempt from inappropriate use of power. These observations led the authors to explore the concept and impact of power in physician leadership. Drawing from a range of conceptualisations including structuralist (French and Raven), feminist (Allen) and poststructuralist (Foucault) conceptualisations of power, we explore how power is acquired and exercised in healthcare systems and enacted in leadership praxis by individual physician leaders (PL). Judicious use of power will benefit from consideration and application of a range of concepts including liminality, power mediation, power distance, inter-related use of power bases, intergroup and shared leadership, inclusive leadership, empowerment, transformational leadership and discourse for meaning-making. Avoiding abuse of power requires moral courage, and those who seek to become accountable leaders may benefit from adaptive reflection. Reframing ‘followers’ as ‘constituents or citizens’ is one way to interrupt discourses and narratives that reinforce traditional power imbalances. Applying these concepts can enhance creativity, cocreation and citizenship-strengthening commitment to improved healthcare. PLs can contribute greatly in this regard to further transform healthcare.
- clinical leadership
- medical leadership
- health system
- improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Power is an inescapable aspect of physician leadership. The word ‘power’ may have negative connotations for some, but power and leadership are intimately related and both contribute to achieving organisational outcomes. Although in healthcare leadership is widely discussed and studied, the concept of power and its impact have received considerably less attention.
There are at least four areas where power by physician leaders (PL) comes into focus. Efforts by physician organisations to gain influence for physicians in healthcare governance demonstrate how power can be simultaneously exerted and extended. While such efforts are generally framed in altruistic terms (eg, by quoting studies that suggest physician leadership correlates with better healthcare outcomes), it is important to recognise that other motivations may exist including a desire to reassert physician power and reclaim traditional status and roles. Similarly, the expectation of physicians to act as stewards of high value, cost-effective care can provide a rationale for increasing the decision-making authority of physicians in the healthcare team. How complex power dynamics affect interprofessional (IP) healthcare (education and practice) at both the systems level and at the point of care is frequently left unaddressed. Power also shapes the profession’s attempts to address physician and learner well-being with its implications for patient care.
These realities, and the fact that power remains ill defined in the medical context, suggest that more dialogue about power is needed. Shifts in power are reshaping the landscape of healthcare governance and IP collaboration, with implications for multidisciplinary team function, system transformation and patient care. These developments have led some to question whether pre-existing discourses on power and physician leadership in healthcare need to be revisited. These are discussions, which can be expected to generate tensions, both within the profession and between professions.
In this paper, we explore the conceptualisation of power and examine how it reflects PL behaviour and healthcare governance, and organisational decision-making. Drawing on existing leadership theories, we offer an alternate perspective on physician leadership that acknowledges power and expands its conceptualisation, ultimately seeking to both mitigate and leverage the effect of power for the benefit of the healthcare system and patient care. Specifically excluded from this discussion are the power dynamics in the physician–patient relationship, which represent an additional layer of complexity.
Power and influence in healthcare
There are many conceptualisations of power that can be drawn from philosophical, social and psychological perspectives. The terms power and influence are often conflated and it may be helpful to use the terms power and influence as separate entities. It can be suggested that power is the ability to get what one wants even in the face of resistance1 while influence is the ability to get what one wants even in the absence of fear of punishment or promise of reward.2
There are three main conceptualisations of power. The first and perhaps the most commonly held conceptualisation of power is the structuralist view of power-over others to achieve compliance.3 The structural elements of power captured in French and Raven’s framework include coercive, reward, expert, legitimate, referent and information power bases.4 5 The first two (coercive and reward) are sometimes referred to as hard power and the remainder as soft power.6 Leaders access and build their power bases to accomplish their goals. While this framework represents a widely accepted view of power, many consider it incomplete due to its emphasis on the leader, lack of social-cultural contexts and failure to address ‘followers’ choices.’ The second is a feminist view, which incorporates power-to (empowerment) and power-with (collective ability to act based on reciprocity and receptivity) and conceptualises power as the ability to work together in concert.7 This perspective is more consistent with the term’s Latin roots (potere) and the French word (pouvoir), both of which mean, ‘to be able.’ It is relevant to addressing equity gaps in medicine and healthcare, enriching medical education and enhancing multidisciplinarity in patient care. The poststructuralist Foucauldian perspective is the third perspective. It addresses the mechanics of power postulating ‘power being constituted through knowledge’ and explaining how discourses are used to normalise and marginalise in societies.8 According to this perspective, power is a force with both negative and positive impacts and is available to anyone—not just the leader. This concept helps explain the process of internalisation in organisations (alignment of employees’ and organisations’ goals) and provides insights into the use of discourses to create meaning, lead change and manage resistance.
Power plays a key role in organisations9 and together with influence is a tool for leaders to produce desired outcomes.10 An important consideration in applying theories of power to healthcare is the particular way in which clinical work is organised. It has been observed that healthcare organisations (HCO) function as ‘professional bureaucracies’ within which the expertise and knowledge of the professionals determine the degree of control (or power) an actor or group of actors can exert over service delivery.11 In contrast to ‘machine bureaucracies’ work autonomy within professional bureaucracies is externally regulated by professional bodies and not by internal management structures. Healthcare delivery therefore includes inverted power structures, where front-line healthcare workers (can) exert greater influence over their daily decision-making than those in formal positions of authority who are nominally responsible for managing operational services.12 13 This organisational structure in healthcare delivery and education distributes power between the titled leaders and the professionals throughout an organisation. As a result, significant clinical change in an HCO is impossible without the cooperation and support of clinicians at all levels.
The evolution of healthcare systems from provider-centric to patient-centric integrated systems elicits multiple issues relevant to the use of power. Implored by the need for better access, higher quality care and enhanced efficiency, this integration14 is aimed at creating coherence and collaboration within healthcare system, through alignment of fiscal, administrative and care delivery aspects.15 Given the key role of physicians in service delivery and somewhat limited impact of unifying fragmented care through regionalisation (which involved limited physician leadership),16 the role of physician leadership in developing and delivering integrated care appears obvious but has also been identified by others as an essential attribute.17 Increasingly, calls for leadership by clinicians (particularly physicians) are framed as a moral obligation, and explicitly articulated as an aspect of social accountability18 through claims that healthcare outcomes are better with physicians in leadership positions.19–21 In some sections of the physician community including some physician professional organisations there is now a belief in the centrality of leadership by physicians in healthcare transformation.22 However, reclaiming leadership23 can also be seen as an exercise in power and influence. The challenge is that the healthcare system requires collaborative leadership,24 which necessitates enhancing physician leadership; while at the same time, the actual exercise of collective (shared) leadership25 requires that PLs would need to become comfortable with sharing power appropriately.
At times, tension exists between the profession’s efforts to extend influence and the disinclination of many in the medical community to recognise and be accountable for physician power as it currently operates in HCOs. Although the expectation of resource stewardship by physicians can theoretically extend physicians’ control over resources, reluctance by some physicians to attribute unnecessary care to their own behaviours has been identified as a barrier to the implementation of resource stewardship measures such as Choosing Wisely Canada.26 The belief held by many physicians that it is not their responsibility to reduce healthcare costs27 has implications for the exercise of power by PLs.
Challenges in IP practice and IP education frequently arise from entrenched attitudes and inflexible professional identities that reinforce traditional hierarchies.28 29 Despite the current emphasis on teamwork and IP care, many physicians remain deeply rooted in independent day-to-day practices, and have not adopted the mindset needed for effective collaboration.
A newer, less obvious arena for the exercise of power is the burgeoning physician wellness movement. Restriction in duty hours and the pushback against traditional medical training can be seen as a shift in the power differential between learners and established physicians who trained in the older system. Decisions to practise in a way that supports wellness can represent the reclamation of personal power for individual physicians. The narrative on physician well-being is expanding concepts of physician burnout and resiliency by reframing these in terms of moral injury (witnessing, perpetuating or preventing behaviours against one’s values, morals and expertise)30 and even human rights violations of physicians and learners.31 This narrative is also shifting the discussion from individual focus to include systems that enforce such behaviours, questioning core values such as compassion32 and restoring meaning and purpose of the profession, for the individuals and medical education. Although the evidence for the specific link between organisational leadership and well-being is moderate,33 leadership interventions at an organisational level have been shown to be beneficial in improving physician well-being.34
Physician leaders and power
Current realities
Physicians exercise and manage power by drawing on the multiple bases of power to which they have access.35 See table 1. Physicians hold expert power associated with their professional status by virtue of their knowledge, skills and abilities. Traditionally, they have also possessed information power, although the accessibility of information with technological advances has diminished this. Some may even have referent power, which is based on character, relationships and reputation. The current trend of seeking wider and legitimate power as stewards of healthcare systems makes access to reward and coercive power bases inevitable.
Power bases and their relation to outcomes76
Physicians demonstrate an appropriate and responsible use of power (and influence) when it is for individual or collective patient care. For example, the surgeon who is able to add an emergency case to an overbooked operating room schedule is using her power to fulfil her social contract. Other members of the healthcare team may choose to respect and facilitate this enactment of power when it is in the best interest of the patient. However, if the advocacy for resources for an individual patient is autocratic or unintentional, it may undermine the collegial relationships and well-being of the team. In contrast, power can also be used inappropriately when, for instance, the same surgeon modifies schedules for her own convenience. In both cases, the care of other patients may be negatively impacted if the result is decreased team function.
Abuse of power may be rationalised by the leaders in terms of achieving desired outcomes, especially in organisations without clear policies that support impartiality. PLs with titled roles may consciously or unconsciously bias decision-making processes within the organisation. A department chair who exercises power to affect the decision of a search committee, which should act autonomously, may rationalise the action as necessary to get the ‘best high-potential candidate.’ The candidate, if appointed, may perpetuate this authoritarian/coercive style.
An association exists between narcissism and leadership, with narcissists seeking positional leadership more often and frequently being identified by others as having leadership qualities. Some qualities of narcissists are desirable, such as a propensity towards innovation in a rapidly changing field; however, leaders with narcissistic motivations around power and inclinations towards hubris may show the least compunction about inappropriately exercising power, which can then have devastating effects on their organisations.36 Insecure PLs with low insight may have maladaptive responses to perceived criticism and may become trapped in a vicious cycle of insecurity and injury to self-esteem, which then increases the risk of further misuse of power to maintain or defend one’s leadership position. At the extreme end of the spectrum are leaders with psychopathic or Machiavellian personality styles. Psychopathy, narcissism and Machiavellianism have been termed ‘the dark triad’, and leaders with these personality types have what has been described as a ‘chaotic and precarious managing style’ that can destroy meaning and purpose in a workplace.37
Recognition of the potential for misuse of power has led to the creation of codes of conduct (eg, Hippocratic Oath, Canadian Medical Association/American Medical Association Code of Ethics and the General Medical Council’s Good Medical Practice) and professional standards. Yet, these are sometimes transgressed and not always enforced in day-to-day practice. The actions of role models and teachers may constitute a hidden curriculum about physician power that contradicts the formal curriculum emphasising collaboration. Their tacit messages and unspoken values can influence learners, who go on to exercise power in the same manner as their teachers.38
How it ought to be
For practical and moral reasons, physicians would benefit from learning to responsibly use power. Understanding the concepts of power described above (the structuralist—identifying and managing power bases; the feminist—challenging leaders to be more inclusive; and poststructuralist—using knowledge to construct narratives and discourses) is a useful first step, and topics related to leadership and power should be incorporated into faculty development and medical training at all levels. In addition, there are strategies that may be used to help physicians recognise, accept and optimally leverage their power to support the functioning of complex organisations and improve patient care.
Becoming comfortable with the use of power and transcending liminality
Many physicians and PLs are uncomfortable with the idea of power and find it difficult to acknowledge and use power. It is not uncommon for PLs to talk about feeling like ‘imposters’ when they assume leadership positions.39 The term ‘liminality’ describes the process of transition as well as the emotional state associated with it.40 PLs who accept titled roles may find themselves in a liminal state, caught in the ‘betwixt and between’ space where they exercise the values and standards of both the clinical and the administrative worlds.41 The change in roles and responsibilities from informal to formal power can involve responsibilities and actions that are in conflict with the perceived needs and goals of the individual, or in contrast with their previous professional identity. Discomfort with new formal power may therefore cause leaders to resist and deny this change. However, acknowledging the power inherent in the position is the first step in understanding how to use power to deliver on the position’s mandate. Insecure leaders may succumb to seeking approval for routine decisions leading to delays, unnecessary meetings and doubtful constituents leading to lowered confidence in their leadership. If there is to be hope of mitigating the negative effects of misused power, reflective PLs will need to embrace their new leader identity and move beyond the liminal state.
Acting with integrity to build connections and relationships
Followers can and do create constraints for leaders. Power is mediated by peers’ and followers’ perceptions concerning the fairness with which leaders use power.42 Individuals may respond to leaders based on their own expectations of the leaders and past experiences of power. These factors can be as influential as the reality of the situation, especially if there are problems with trust in the relationship. Therefore, it is important that leaders seek to understand those receiving direction and how they will be motivated to cocreate, collaborate, follow or resist. Addressing these motivations, fostering dialogue, attending to perceived threats and incorporating meaningful rewards could help improve alignment between leaders and constituents. We have slightly modified Yukl’s elaboration of French and Raven’s framework (table 1), which can be used for reflection on how power can optimise outcomes and mitigate harm. There is also a seventh base of power, ‘the power of connections,’ that supports change through influence by proxy-political coalitions alluded to in the Lead Self, Engage Others Achieve Results, Develop Coalitions and Systems Transformation (LEADS) framework that guides exercise of moral power.43
The feminist perspective of power as the collective ability to act in concert7 highlights the exercise of power through connected networks44 and navigating organisational politics (an integral component of organisational dynamics) by seeing politics as power in action.45 Leaders will benefit from presenting change initiatives in an inspiring manner. Commitment and cocreation are more likely if the proposed change is congruent with expertise, time requirements seem reasonable and a high change/effort ratio appears likely. Conversely, opposition can be expected if the outcome is deemed improbable and time demands excessive.
Understanding power bases
Individuals have a combination of power bases: personal (referent and expert) and organisational (legitimate, reward, coercive and information). Leaders select between these by taking into account personal and social (context, needs, people) factors. Legitimate power, while often the most obvious form of power to external observers, covers only a narrow range of influence with boundaries that are inappropriate to overstep.46 Since these power bases are inter-related, the use of one may affect the use of the other. For example, expert power may enhance legitimate power, while use of coercive power may reduce referent power. PLs should be aware that sometimes, soft power may be insufficient, and will be more effective if it is perceived to be backed by hard power. However, the rare situations where the use of authoritarian power is essential (physician discipline47 or quarantine during outbreaks) should be followed by consultation and re-evaluation. ‘Just the right amount of’ assertiveness is crucial as neither too much nor too little is effective over time.48
Creating a right mix of power relationships
The concept of power distance49 refers to how people from different cultural backgrounds, organisations and societies expect and agree to unequal distribution and sharing of power between leaders and followers or constituents. HCOs are both situated in societal cultures and possessed of their own organisational cultures. With increasing cultural diversity in the healthcare workforce, leaders must be aware of how people perceive and react to formal authority. Those who expect a low power distance with flatter hierarchies and less power differential may not react well to a high power distance management style that is more directive and authoritarian. Healthcare governance can cocreate organisations for optimal patient care, whether these be low-power, distance-flat organisations or high-power, hierarchical and centralised organisations. Diversity of thought and talent is known to promote better workplace performance and higher engagement with the organisation. An inclusive leadership perspective50 incorporates respect for diverse viewpoints, facilitating dialogue, serving traditionally under-represented constituents and ensuring careful attention to both privilege and subjugation. Incorporation of feminist perspectives and theories would enrich the strategies for achieving equity, diversity and inclusiveness in health professions education and healthcare delivery.51 52
Planning and executing shared power structures
Sharing power can be a strong and authentic leadership approach. PLs of larger segments of healthcare (with constituents from multiple healthcare professions) may lead diverse groups across multiple intra/interorganisational boundaries, and may serve in dyadic leadership models with coleader backgrounds in administration or other healthcare professions. In these shared/collective leadership situations PLs will need to share power with their dyad partner and also avoid being perceived as leaders who only advance physicians’ interests.25 53 Heifetz’s conceptualisation of targets of power as ‘citizens’ and ‘constituents’ instead of followers54 changes the perspective on the relationship between the leader and the ‘led.’ Based on concordant values, transformational leadership enhances motivation and morale, inspiring those being led to perform at their best and helping to bring leaders and constituents closer together. Transformational leadership helps connect leaders’ visions and actions with their ‘followers’ sense of identity through role modelling, ownership of their work and alignment with organisation’s vision.55 Empowering members of the organisation, enhancing trust and promoting psychological safety are ways that leaders can help others reach their full potential56 and achieve organisational outcomes. Empowerment is a prerequisite for shared, distributed and collaborative leadership models where power itself needs to be shared for joint accountability.57 However, empowerment needs to be balanced with the need to maintain a differential identity between leaders and constituents that recognises the leader’s responsibility to steer the organisation and its constituents towards desired outcomes.
Designing environments and processes that influence behaviour
The Foucauldian perspective8 emphasises the way that leaders use their power for meaning-making. This includes both systematic changes as well as using discourses to shape the thinking of healthcare workers. For instance, PLs successfully spread their influence when they design systems that lead towards cultures of safety and help create organisations that embrace inclusivity and diversity. Relational cultural theory informs healthy coexistence in societal structures through its ‘five good things’ (sense of energy, increased sense of self-worth, increased clarity, ability and motivation to take action, and desire for more connection) required for ‘growth fostering relationships.’58 These changes then hold the power to influence all constituents in the organisation as they come to know ‘the way we do things around here.’ PLs can enhance the positive effects of power by demonstrating behaviour that is in alignment with their change initiatives. They may negatively impact their change initiatives if they do not take into account the emotions and perspectives of others (explained through the Status, Certainty, Autonomy, Relatedness and Fairness (SCARF) model of human social experience and includes status with respect to others, certainty about the future, autonomy, relatedness with others and perceptions of fairness in interactions),59 view others as tools for their own purpose, punish or exclude people for dissenting opinions and ideas, become overconfident or take unnecessary risks on behalf of others. To foster change and demonstrate a balanced approach, PLs must be inclusive of dominant and non-dominant discourses being cognisant of both rights and justice to construct narratives that are truly evidence informed and not biased in favour of the medical profession.
With the gradual shift in the narrative on physician well-being from surface understandings (physician burnout, self-reported measures of wellness, behavioural interventions aimed primarily at individual level) to deeper considerations (framing the phenomena in terms of moral injury and human rights violations) interventions at cognitive and affective levels may seek to reconnect physicians with the core values of the profession such as compassion, and restoring the meaning and purpose of the profession as healers.60 Medical education61 and transformation of individuals and institutions62 for social responsiveness and social justice require a balanced approach to the exercise of power at global and local levels. PLs would benefit from adopting evidence-based practices on leadership interventions such as enhancing autonomy and relatedness at systems level to enhance physician well-being34 and to include physician wellness as a health system quality indicator.63
Avoiding the abuse of power
Power can corrupt and leaders can go astray when they use power for their own gains.64 The exploitation of others for personal goals through actions such as withholding important information, or excluding efficient group members is more likely when the leaders have a ‘dominance’ motivation and perceive their power to be tenuous especially in unstable or transitioning organisations.65 Even in the face of managerialism (regulation and control of professional work by managers), physicians are often able to maintain strong voices due to their expert power.66 Because of this, there are definite risks that scientific bureaucratic medicine can become too entrenched when the managerial and expert power bases come together in the hands of one profession. On the other hand, there is evidence that qualified PLs/managers are not always full participants in decision-making processes,67 suggesting that this may not be a concern in the majority of situations.
Quis custodiet ipsos custodes—who watches the watchmen?
Juvenal’s Satires raised the question of how to ensure the accountability of those in power, which haunts all hierarchical power structures. Hierarchy and power are self-evident in the practice of medicine.68 PLs may need to manage both their power and that of the other physicians. These PLs, like all physicians, are bound by a social contract, which grants them power and status.69 In return, they must have the moral conviction to uphold high ethical standards and regulate themselves and their peers.
However, PLs are carved from what Immanuel Kant called ‘the same warped wood of humanity’ as everyone else70 and are just as fallible. A single approach to accountability is not likely to be appropriate for all hierarchical levels of leadership. The familiar strategy of defining roles, expectations and metrics in an organisational reporting structure risks reinforcing hierarchy without improving accountability.71 A more radical and transformative strategy would require PLs to develop a network of peers to comanage accountability. Strategies might include ‘leadership issues’ rounds, where challenging situations or difficult decisions are discussed. Incorporating ‘liberating structures’ would develop a culture of psychological safety. The attendant transparency and feedback would create a possibility of surfacing that which people would otherwise feel inhibited to share. The goal would be to transform the culture of the solitary, authoritative powerful figure concealing errors to avoid embarrassment to a collaborative group of non-judgemental colleagues who can help improve decision-making.
Implications and conclusions
It is our view that physicians should discuss, understand and use sound judgement regarding the complex, intertwined concepts of power and leadership. As they accept greater roles in healthcare governance and administration they should be held to higher standards than as individual practising clinicians. Power will be used by leaders, but as Gini has asked,72 ‘will it be used wisely and well?’
The prudent use of power by PLs requires thoughtful attention to multiple factors (figure 1). At the individual level, staying authentic to oneself and connecting to personal values may make it more possible to exercise moral courage. PLs will need to transcend liminality, resist narcissism and hubris and show the capacity to use feedback on their leadership through adaptive reflection. Many of these concepts have been incorporated into what is termed ‘person-centered leadership’, an approach which attends to the psychological dynamics, values and needs of the individuals within the organisation. In person-centred leadership, the well-being of patients and staff is both relevant to creating a compassionate and sustainable healthcare system.73
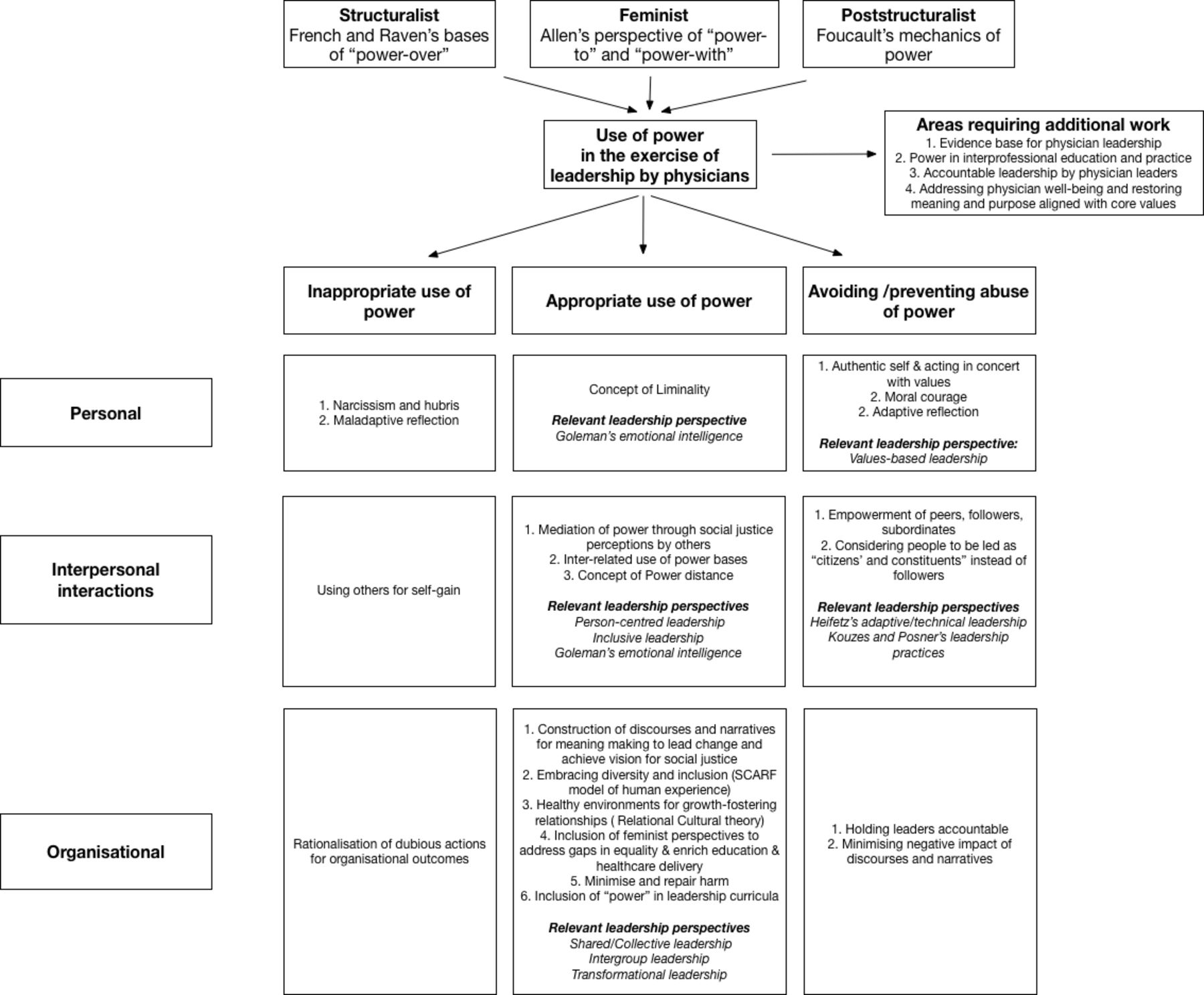
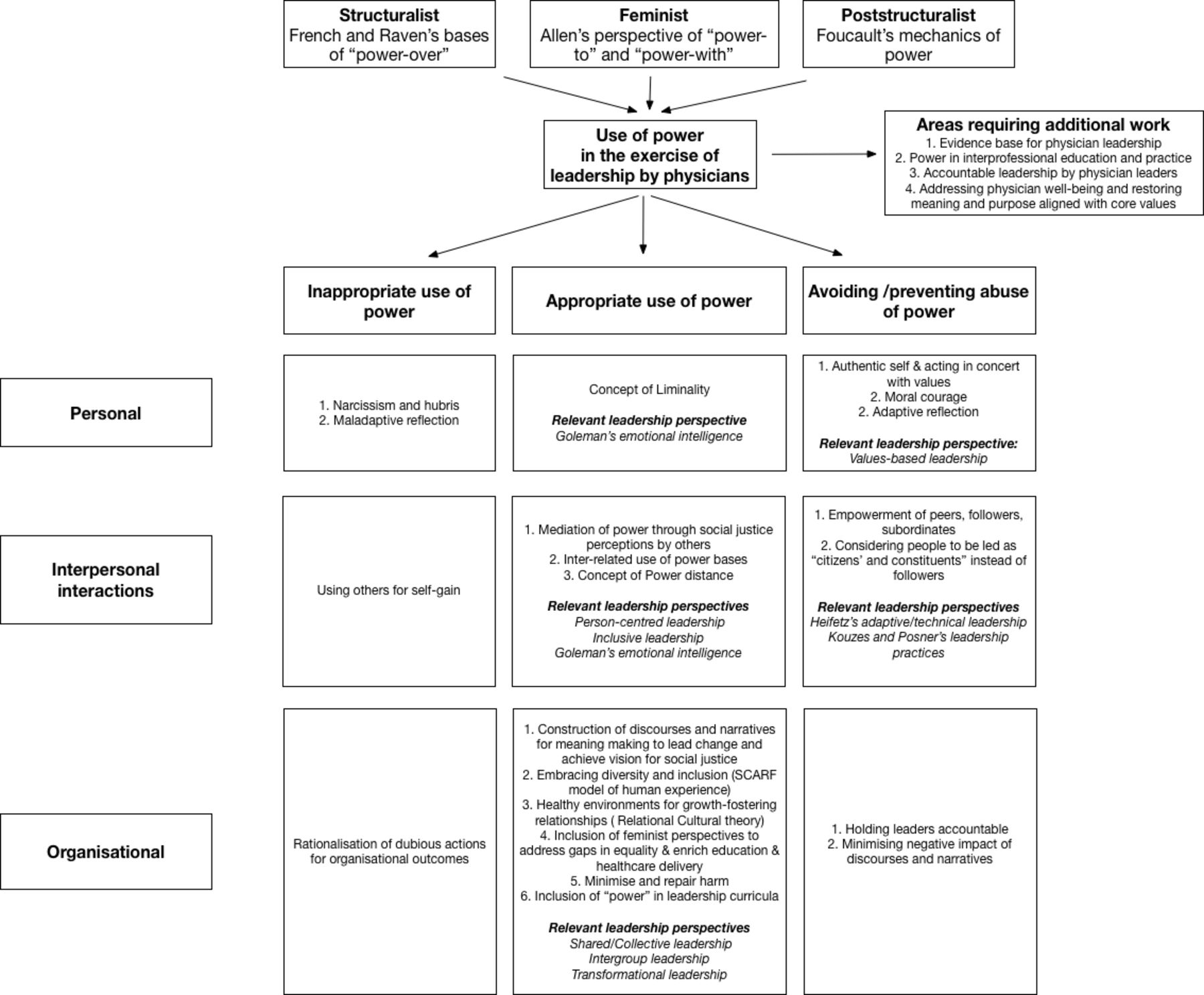{kind=link}
Concepts and principles informing utilisation of power for leadership by physicians.
Interpersonal interactions will benefit from considering those who are led as citizens and constituents (instead of followers) and resist using others for self-gain. Empowering the constituents (power-to and power-with) can lead to effective collaborative patient care. Translating underlying principles (power mediation through perceptions of social justice, power distance and inter-related uses of power bases) would be associated with effective leadership. Goleman’s concept of emotional intelligence74 and Kouzes and Posner’s practices of leadership75 provide practical guidance on elevating interpersonal interactions in an authentic manner. Leadership training and coaching for PLs, including how to seek and incorporate feedback, should explicitly include a discussion about power in order to prepare them for their expanded roles.
At the organisational level with increasing leadership roles in healthcare, more PLs will lead larger groups of diverse workers from all healthcare professions. For this, the principles and practices of inclusive, transformational, shared/collective and intergroup leadership and high levels of accountability are required. Great leaders limit harm done in achieving outcomes and repair inadvertent or unavoidable harms. Fostering a new form of dialogue with other constituents, one that minimises the negative impact of traditional discourses and narratives, will be key as PLs seek to change the landscape of healthcare delivery. As we train the next generation of PLs, we need to overcome a hidden curriculum that reinforces traditional hierarchies, where dissent is often silenced, and power is ineffectively distributed.
This paper highlights the need for additional work in both research and praxis explicitly addressing power in IP and multidisciplinary care, developing robust mechanisms for assessing leader impact and accountability and addressing global issues core to the profession to reclaim meaning and purpose consistent with our core values. A complex adaptive system such as healthcare requires collaborative leadership and thus sharing of power, and ultimately this may be where the greatest hope for progress can be found; not through attempting to eliminate or deny the existence of power, but in identifying, understanding and distributing it throughout systems in a fair and effective manner. Although it is a cliché, it is nonetheless true that with great power comes great responsibility. It could also be said that with shared power and responsibility, there lies the potential for greatness.
References
Footnotes
Correction notice This article has been corrected since it was published online first. The spelling of "Physician" is corrected in the heading "Physician leaders and power".
Contributors All coauthors (AS, DM, LH, DD, DAB, MKC, AM and JB) are responsible for the idea and were involved in writing and editing (narrative comments and generating a consensus opinion, reviewing first and subsequent drafts and the final version) of the paper. AS and JB were overall leads and are responsible for the overall content as guarantors. AS submitted the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.