Article Text

Abstract
Introduction and background Like many health systems in low-income and middle-income countries, the South African health system has failed to decrease both maternal and perinatal mortality significantly, especially in district hospitals. Inappropriately trained healthcare providers and poor clinical leadership are repeatedly linked to healthcare providers’ preventable factors contributing to most maternal and perinatal deaths. Clinical skills of healthcare providers have been largely addressed, while clinical leadership remained neglected. One strategy implemented recently to support clinical leadership is the introduction of District Clinical Specialist Teams (DCSTs). Clinical leadership in the labour ward of district hospitals in KwaZulu-Natal (KZN) is conceptualised as an emergent phenomenon arising from dynamic interactions in the labour ward and the broader health system, converging to attain optimal patient care.
Aim To evaluate the enablers and barriers to clinical leadership in the labour ward of district hospitals.
Method Iterative data collection and analysis, following the Corbin and Strauss grounded theory approach, was applied. In-depth interviews were carried out with the midwifery members of the DCSTs in KZN. The emergent enablers and barriers to clinical leadership were presented and discussed at a workshop with broader midwifery representation, leading to a final classification of enablers and barriers to clinical leadership.
Results and conclusion Enablers and barriers to clinical leadership arise as a result of emergent dynamic interactions within the labour ward and the broader health system, located at policy, organisational, team and individual healthcare provider levels, with the policy context as the overriding factor framing the implementation of clinical leadership.
- grounded theory
- clinical leadership
- enabler/barriers
- South Africa
- teamwork
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The South African health system is undergoing reform reflecting the state of many other developing health systems in low-income and middle-income countries (LMICs).1 2 Like many health systems in LMICs, the South African health system has failed to decrease both maternal and perinatal mortality significantly, especially in district hospitals, a primary level of care, offering comprehensive essential obstetric care.3–8 The persistent maternal and perinatal mortality in South Africa is attributed to poor or lack of leadership at country, district and institutional levels.9 10
In district hospitals, inappropriately trained healthcare providers and poor clinical leadership are repeatedly linked to healthcare providers’ preventable factors contributing to most maternal and perinatal deaths.11–13 While clinical skills of healthcare providers have been largely addressed, clinical leadership remained neglected.12 14–16
Recently, the National Department of Health introduced District Clinical Specialist Teams (DCSTs) as a strategy to improve maternal and child outcomes in district hospitals, through the provision of support for clinical leadership and governance.17 However, the provision of support by DCSTs is an outreach activity from district health offices, where the DCSTs are located, to district hospitals.
In district hospitals, a hierarchy of positional leaders is overall responsible for ensuring clinical leadership. However, the actual provision of clinical leadership at the bedside has been found to be inadequate and ineffective.12 18–20 Thus, the provision of clinical leadership within district hospitals requires development and strengthening.
In the labour ward of district hospitals, most deliveries are midwife-led, with doctors on call to deal with complications and emergencies.21 Midwives are equipped with the necessary skills to make clinical decisions pertaining to mothers and babies; and should be able to influence care practices at the bedside, and to contribute to effective teamwork and the creation of an enabling work environment.21–23 But, often, midwives are neither clear about, nor have been prepared for, the clinical leadership role.24 25 To enable midwives to provide effective care, it becomes imperative that they understand the clinical leadership role.24
Clinical leadership in the labour ward of district hospitals in KwaZulu-Natal (KZN), South Africa, has been conceptualised as an emergent phenomenon arising from dynamic interactions in the labour ward and the broader health system, which converge to attain optimal patient care.26
However, the enablers and barriers to the realisation of this conceptualisation of clinical leadership are not well understood.
Aim
Given the need for the development of clinical leadership in the labour ward of district hospitals in KZN, South Africa, this study was designed to evaluate the enablers of, and barriers to, clinical leadership.
Methods
Study design and respondents
A grounded theory methodology according to Corbin and Strauss27 was used to evaluate enablers and barriers to clinical leadership in the labour ward of district hospitals. This methodology seeks to generate evidence for a phenomenon where there is little available evidence,27 28 and was considered most appropriate in a context where there is a paucity of evidence on the implementation of clinical leadership.
Purposive heterogeneous sampling was implemented to recruit the research participants. Advanced midwifery members of the DCSTs in KZN were selected because of their role in supporting clinical leadership. Advanced midwives in leadership positions in labour wards of district hospitals, academicians responsible for midwifery training in KZN, and district and provincial level representatives from the KZN Department of Health were selected to elicit data from their respective perspective on the enablers and barriers to clinical leadership. The researcher (SM) recruited respondents via telephonic and email invitation.
Procedure
The study was conducted in two phases:
In Phase I, the researcher (SM) conducted individual in-depth face-to-face and telephonic audio-recorded interviews with eight advanced midwifery members of the DCSTs, in a location of each respondent’s choice. Interviews were conducted in English and lasted between 45 min and 1 hour. An interview guide using open-ended questions guided the in-depth interview,29 covering enablers and barriers to clinical leadership.
In keeping with the Corbin and Strauss approach to grounded theory, data collection and analysis happened iteratively.28 After each interview, transcripts were analysed in three stages. In open coding, transcripts were read and re-read, assigning labels to chunks of data. In the stage of axial coding, codes with similar meaning were grouped together, as were codes that were related to each other. The stage of selective coding led to the identification of major enablers and barriers to clinical leadership. Phase I resulted in the classification of enablers and barriers to clinical leadership at the individual, team, organisational and policy levels.
In Phase II, the authors facilitated a workshop to provide feedback on Phase I of the study and to generate additional insights. Workshop participants comprised all the interviewed advanced midwifery members of the DCSTs (8), advanced diploma midwives in leadership positions in labour wards of district hospitals (5), academicians responsible for midwifery training in KZN (2), and district (1) and provincial (1) level representatives from the Directorate for Maternal, Child and Women’s Health in the Provincial Department of Health.
In the workshop, summarised feedback on enablers and barriers to clinical leadership was provided by the authors and discussed by all present. The workshop was video recorded. The researcher (SM) listened to the recording many times to identify consensus and divergence on the enablers and barriers to clinical leadership identified in Phase I, as well as to discern different emphases provided by the workshop participants. SM analysed the audio recording of the workshop with a focus on attaining meaning saturation for the categories identified in Phase I.30 31 Further, the workshop assisted in ensuring trustworthiness of the research findings by introducing member check as a technique for enhancing credibility.32 Additional measures to ensure the trustworthiness of the study33 is summarised in table 1.
Measures for ensuring trustworthiness
Results
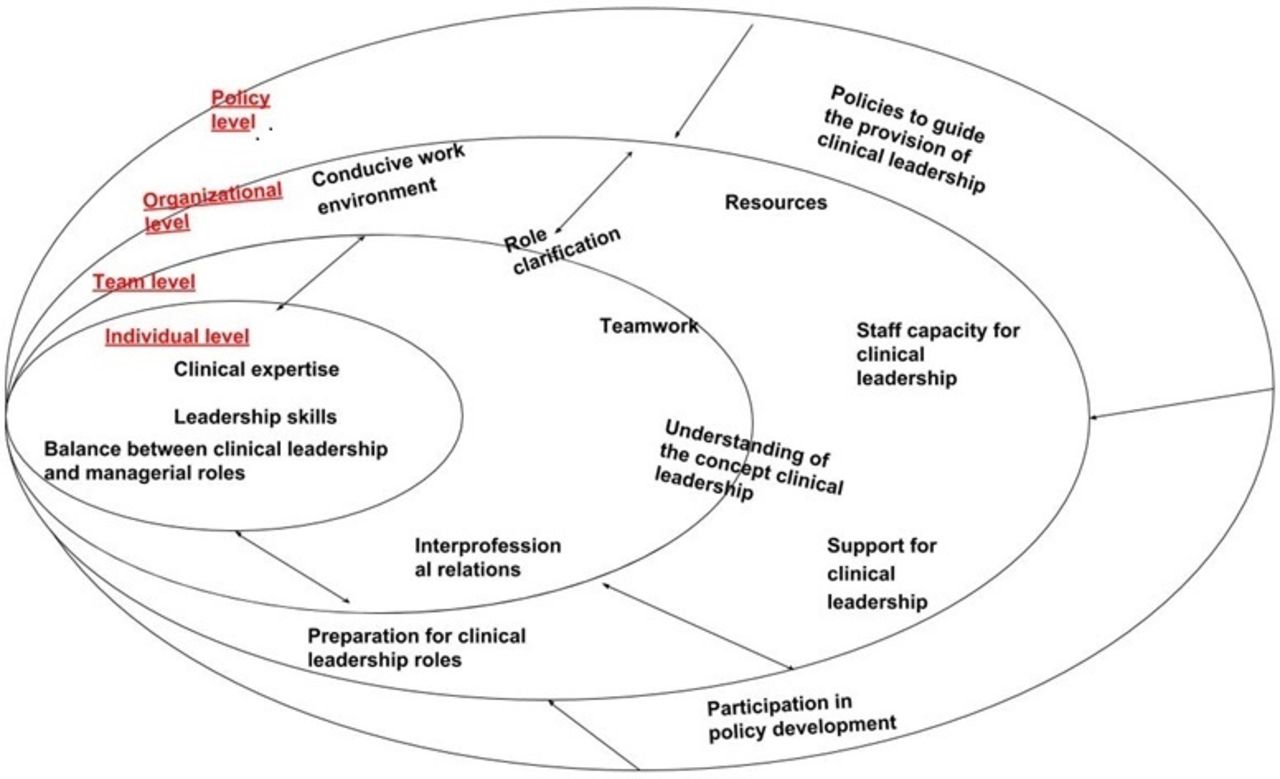
Enablers and barriers to clinical leadership in the labour ward of district hospitals in KZN were identified at policy, organisational, team and individual levels, as reflected in figure 1. The factors identified at the different levels can be either enablers or barriers, depending on whether they are present or not. Although presented separately, the enablers and barriers within and between levels are linked, with much overlap between them.

{kind=link}
Summary of enablers and barriers to clinical leadership in the labour ward of district hospitals in KZN, South Africa, in 2015. KZN, KwaZulu-Natal.
Enablers and barriers to clinical leadership at the policy level
Respondents identified the need for a policy context that supports clinical leadership in the labour ward of district hospitals. Policies are required to guide the training and development for the clinical leadership role. Respondents emphasised the importance of involving clinical leaders in policy development processes to ensure implementation.
Midwives need to be included in policy development; in this way, they are able to ensure that they understand them and use them. (Respondent 7)
When policies and guidelines are developed, clinical leaders need to input on them. … if you engage them (clinical leaders) while you are still developing them (policies) to say: ‘guys have a look at these policies/guidelines, do you have any input?’ This will ensure that they know the policies and implement them. (Respondent 5)
Enablers and barriers to clinical leadership at the organizational level
Factors identified at organisational levels ranged from the work environment, service organisation and staff capacity for clinical leadership, support and preparation for the role.
The physical workspace and resources
The work environment, defined in terms of availability of training and education equipment that supports the development of leadership skills, was seen to underpin effective clinical leadership at the bedside.
You need an environment that is conducive to provide clinical leadership. But the environment is not welcoming. (Respondent 4)
Clinical leadership is constrained because there are no resources to develop clinical leadership. (Workshop participant)
Service organization
The organisational context was identified as influencing clinical leadership. Particularly, the shortage of formally appointed clinical leaders was perceived to hinder the provision of effective clinical leadership.
A maternity service in a district hospital is headed by the medical manager. The maternity service, in turn, is divided into wards, for example, antenatal and labour wards, each headed by an operational manager or midwife formally appointed as a clinical leader. (Workshop participant)
There are shortages of formally appointed clinical leaders to all the divisions within maternity, hindering formally appointed clinical leaders to provide effective clinical leadership at the bedside.
I am an operational manager for maternity, which includes antenatal care, nursery, labour ward, postnatal care and high-risk patients. It is not possible for me to provide 100% clinical leadership in an environment like that. (Workshop participant)
Additionally, respondents identified the need for proper equipment for training and development, for the clinical leadership roles at the bedside.
You need proper equipment to provide clinical leadership. You can’t expect effective leadership if there is no equipment (for training and development of leadership roles). (Respondent 4)
Staff capacity for clinical leadership
High-staff turnover was seen to not allow sufficient time to develop clinical expertise in midwives, limiting shared clinical leadership at the bedside. Even after being equipped with the required skills, healthcare professionals are leaving the labour ward in search of better opportunities, or for fear of litigation, making it difficult to retain skilled healthcare providers. Further, it is not always easy to recruit new healthcare providers due to restrictive recruitment procedures.
There is a fast movement of staff. After you have equipped them (staff) with the required skills, they leave for greener pasture. If you (clinical leader) do not have a stable staff, you are unable to make progress. It is a vicious circle that you are not able to break, not having the quality of staff you desire. (Respondent 3)
Recruitments procedures are difficult because posts are frozen, you cannot get the staff you need, especially in rural areas, and if you get them for 3 months they leave for greener pastures. (Respondent 2)
Support for the role of clinical leadership
Midwives indicated that support from health service managers enabled clinical leadership roles. They expressed that supervision and mentoring were necessary to assist clinical leaders in their roles. Midwives also indicated the need for better communication between the management team and the midwives at the bedside, to support clinical leadership.
When I am talking of support, I am talking about clinical support, like when I (positional clinical leader) am visiting the labour ward, we (positional clinical leader and nursing manager) look at the case together; we manage the case together with frontline healthcare providers that are present, so that they will learn. (Respondent 8)
Preparation for clinical leadership roles
Preparation for clinical leadership roles is essential for ensuring effective clinical leadership, especially for formally appointed clinical leaders. Induction, in-service training and formal training programmes were considered important parts of the preparation required for clinical leadership roles. The emphasis on what should be covered in the training fell on leadership skills and clinical expertise. Respondents expressed the opinion that training should be provided prior to the formal appointment to the role of clinical leader. Training and support for the clinical leadership role should also be made available after the appointment of clinical leaders.
I think there should be some clinical leadership training before you assume your role as a (formally appointed) clinical leader. (Respondent 4)
Induction is very important especially on the existing (clinical) protocols, guidelines and all the programs that you are going to be responsible for. (Respondent 6)
I cannot overemphasise … without in-service training or obstetric drills, you cannot provide better care. So in-service education is important in maternity. (Respondent 7)
Enablers and barriers to clinical leadership at the team level
Themes identified at the team level are related to the perceptions of clinical leadership and interprofessional relations in the labour ward.
Perception of the concept of clinical leadership
Midwives felt that clinical leadership responsibilities in the labour ward were not clearly defined, especially for formally appointed clinical leaders, hampering their ability to engage in clinical leadership activities. One respondents stated the following:
What I am realising is that the clinical leadership responsibilities are not clearly defined. You find the operational manager doing more of managerial duties than clinical duties. (Respondent 3)
Poor understanding of the concept of clinical leadership by formally appointed clinical leaders was reported as a result of the terminologies used in job designations.
They (clinical leaders) were appointed as operational managers. Even the term ‘clinical leaders’ only came in force with District Clinical Specialist Teams (DCSTs). When you say, ‘operational manager’, it is equal to the day-to-day running of a department. They (Department of Health) need to change the terminology from ‘operational managers’ to ‘clinical leaders’, then it rings a bell. (Respondent 1)
Respondents reported a prevailing perception that clinical leadership activities fell only within the purview of formally appointed leaders.
I think because the senior managers when they need something in the labour ward, they focus on the one that is having a title and say: ‘Can we have this or that?’ and then other healthcare providers are reluctant to step in as clinical leaders. (Respondent 6)
Interprofessional relations
The nature of the care environment in the labour ward was considered essential to facilitate or hinder clinical leadership.
Communication and teamwork were considered essential in ensuring effective clinical leadership.
We work as a team. We can take turns—sometimes it’s the doctor leading, sometimes it’s a nurse or midwife; so that we can actually achieve quality service delivery. (Respondent 4)
Other respondents, however, identified the lack of interprofessional teamwork and conflict as barriers to clinical leadership. The narrative was strong that decision-making power was with doctors, and doctors did not value midwives’ contribution to patient care at the bedside. Midwives suggested that support from health service managers could assist midwives to affirm their clinical leadership roles among other professionals, especially doctors.
There is friction between doctors and nurses. When you (contribute) something as a midwife, and you do not have a specialisation, doctors do not receive it. Sometimes you have to phone the provincial office for somebody to support you. (Respondent 6)
You know how knowledgeable midwives can be, but most of the power for clinical decisions have been given to doctors. Whatever decision or suggestion you make, just because the doctor was not there, he can delay treatment for the patient. (Respondent 7)
Enablers and barriers to clinical leadership at the level of the individual healthcare provider
At the individual healthcare provider level, two major themes were identified: competencies required for effective clinical leadership, and the lack of balance between clinical leadership and managerial responsibilities.
Competencies required for effective clinical leadership
Two major skill sets were identified as fundamental for effective clinical leadership: first, clinical expertise, and second, leadership competencies. Additional domains of leadership competencies include personal, relational and organisational skills.
It doesn’t have to be you (clinical leader) all the time, but you can delegate, allocate some tasks to the staff in your department. (Respondent 7)
For clinical leadership, you need somebody who has skills for mentorship so that she is able to transfer the skills and knowledge to other people, especially the new people that are coming into the department. (Respondent 4)
Midwives also identified a lack of essential skills as a barrier to clinical leadership.
They (clinical leaders) are to be leading by example even with the clinical expertise, but you’ll find that they lack so much. (Respondent 5)
Clinical leaders need to be confident to provide clinical leadership, but many lack confidence, especially in front of medical doctors. (Respondent 6)
Balance between managerial and leadership roles
Midwives noted that formally appointed clinical leaders struggled to balance between managerial and clinical leadership roles. Some respondents, with workshop participants concurring, responded as follows:
There’s a lack of balance between duties…. Operational managers are more managers than clinical leaders. (Respondent 3)
Management calls you if you do not attend a meeting. You don’t know if you should be in your unit (at the bedside) or listen to management (and be in meetings). (Workshop participant)
Discussion
The transitioning health system of Democratic South Africa prioritised making health services available and accessible to all South Africans.34 35 As health services have become available and accessible, the focus has turned towards ensuring the provision of quality care. It is within the context of ensuring quality care that the call for effective clinical leadership has arisen.34 35 This study sought to evaluate the enablers and barriers to clinical leadership in labour wards of district hospitals in KZN, South Africa.
This study confirms a range of findings already identified in the literature emerging from high-income countries (HICs), where clinical leadership is better developed.36–38 The enablers and barriers to clinical leadership identified in HICs are transferable to developing health systems, such as in the South African context, and in other LMICs.
In this study, enablers and barriers to clinical leadership are reported to arise from emergent dynamic interactions within the labour ward and the broader health system, and are located at policy, organisational, team and individual healthcare provider levels. In a health system that is still maturing,1 2 policies aimed specifically at clinical leadership would provide a broad context and strategy to ensure that frameworks and guidelines exist to guide the roles and responsibilities of clinical leadership, and the training and development required to ensure effective clinical leadership.39–41 Having policies on clinical leadership might help to address the enablers and hindrances identified at each of the levels.
Effective clinical leadership requires an enabling environment of care,42–46 which comprises sufficient and adequately trained core staff supported by essential supplies and equipment to provide basic and emergency care.47 48 An enabling environment enables teams to provide safe, effective and quality patient care, and provides professional development.
Positional clinical leaders are mandated to uphold clinical standards, enable professional development and ensure an enabling environment for optimal bedside care.26 49 50 Visibility is an important relational skill required to ensure optimal patient care.26 51 52 The shortages of positional clinical leaders makes it difficult for the few available positional clinical leaders to be visible in labour wards and to provide effective clinical leadership.25
In this study, it was reported that positional clinical leaders struggle to balance between clinical leadership and managerial roles, consistent with other studies.25 53 The struggle to balance roles may be exacerbated by a lack of policy on clinical leadership training and development, contributing to role confusion, or by increased workloads, resulting from a shortage of health workers, leading to inadequate clinical leadership.25 Midwives in this study supported the view that the title used for formally appointed positional clinical leaders might contribute to a poor understanding of the concept of clinical leadership. Hence, including positional clinical leaders in identifying the enablers and barriers to clinical leadership weighted more on managerial issues, rather than leadership, which might have been identified by frontline healthcare providers, introducing a limitation to the study.
Clinical leaders require support to exercise and develop their clinical leadership roles. Mentoring and supervision empower clinical leaders to apply new skills to clinical situations, and provide an opportunity to share and discuss clinical cases with other professionals, enhancing teamwork and better patient care.54 55 This finding is supported by previous research which acknowledged the role of structural support for the development of clinical leadership skills.50
An environment where all healthcare providers could effectively contribute to patient care was seen to be an essential factor influencing clinical leadership in labour wards.26 Communication and teamwork facilitate cohesion, development of interpersonal skills of the care team and interprofessional collaboration through discussion and reflection on practice.56
Midwives expressed that doctors did not value midwives’ contribution to patient care, which is at odds with labour wards in district hospitals, where most deliveries are midwife-led.21 Additionally, it is at odds with the shared nature of clinical leadership which supports shared values, joint responsibility and mutual trust in patient care.42 57 58In such situations, midwives may become reticent to make the clinical decisions they are empowered to make, diminishing their contribution to optimal patient care.59 60 Hence, the need for clear conceptualisations of clinical leadership and descriptions of clinical leadership roles to mitigate interprofessional conflict and confusion, promote effective teamwork and optimal patient care.42 57 58
Competencies of every individual healthcare provider are required to ensure effective clinical leadership.61–63 The emphasis on clinical expertise to ensure effective clinical leadership is consistent with the emphasis found in other studies.52 64 65 Clinical expertise in every member of the team enables shared clinical leadership and effective teamwork.66 Hence, the need for intentional and proactive clinical leadership development becomes more pronounced in such care settings, consistent with the findings in the literature.22 25 There is also a need for evidence-based models, to inform clinical leadership development.
Conclusions
Enablers and barriers to clinical leadership arise as a result of emergent dynamic interactions within the labour ward and the broader health system, located at policy, organisational, team and individual healthcare provider levels, with the policy context as the overriding factor framing the provision and development of clinical leadership.
Acknowledgments
Special thanks go to Professor Edgar Mhlanga (Provincial Specialist of Obstetrics and Gynaecology, Department of Health, Mpumalanga province) for his comments on the draft of this article.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. The author's name has been changed from "Voce Silvia Anna" to "Anna Silvia Voce".
Contributors SM (University of KwaZulu-Natal) planned the study, conducted interviews, performed data analysis and prepared write-up. VSA (University of KwaZulu-Natal) is the SM’s PhD supervisor who made conceptual contributions and provided technical guidance throughout the writing processes (revising the article). Both authors read and approved the final manuscript.
Funding This paper is part of a doctoral study partly funded through a scholarship from the College of Health Sciences at the University of KwaZulu-Natal.
Competing interests None declared.
Patient consent for publication Not Required.
Ethics approval Ethical approval to conduct the study was provided by the University of KwaZulu-Natal Biomedical Research Ethics Committee (Ref.: BE389/14). Permission to conduct the study was obtained from the KwaZulu-Natal Provincial Department of Health (Ref.: HRKM326/14).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data available in a public repository, https://researchspace.ukzn.ac.za/handle/10413/16336 under CC BY-NC.