Article Text

Abstract
Background/aim This paper summarises and extends information presented at the Lilly Lecture 2017. It is based on the author’s experience and research in working to develop senior leaders in many sectors over the last 30 years. The aim is to provide practical, usable insights into an aspect of leadership capability that is often overlooked in order to enable greater effectiveness in leaders.
Methods The paper draws on the author’s own experience, of the research of Harthill and other organisations working with the concepts that have been labelled constructivist development or more lately ‘vertical’ development.
Results Research, both qualitative and quantitative, points to the need for leaders to develop the meaning-making capacities to deal with increased levels of complexity and ambiguity. Fewer than 5% of leaders across multisectors are seen to develop these capacities.
Conclusion Leaders within the National Health Service are particularly challenged by complex and ambiguous contexts. They need to extend their leadership capacities to be able to lead effectively in such contexts. Leaders today are not being supported to develop these capacities and more needs to be done. There are actions that individuals as well as organisations can take to support this development.
- medical leadership
- capability
- capacity
- strategy
- management
Statistics from Altmetric.com
In over 30 years of working with leaders, I have observed an inexorable movement towards leadership becoming faster paced and more complex—and as a consequence, more pressured. This is particularly evident in the National Health Service (NHS) with its heady cocktail of rapidly changing medical technology, shifting demographics, increasing patient demand and expectations, high levels of political engagement (or interference, depending on your perspective) and budget challenges.
My observations are not unique. Since 2014, the environment facing leaders in numerous contexts has been described with the acronym VUCA.1 ‘It’s a VUCA world’ has become the cry—volatile, uncertain, complex and ambiguous. Most leaders agree that their world is increasingly VUCA and that this creates increased demands on them and their leadership.2
While this provides enormous challenges for individuals and organisations, the good news is that we humans are superbly adaptable and can extend our individual and collective abilities. An exercise I often use with leaders is to ask them to recall a time early in their leadership career, perhaps a decade or two ago, and recall the assumptions, attitudes and skills they operated with at that time. I ask them to compare this with their leadership today and ask ‘What has changed?’ The vast majority report gaining what I would describe generically as ‘increased wisdom’, for example people describe gaining the ability to stand back, to consult with others, to be less egotistical in their decision making, to be willing to be wrong and to ask probing questions.
So the good news is that over time we may gain wisdom; however, many leaders also report feeling overwhelmed by the VUCA-ness of their leadership lives. It is clear from the organisational failings such as that at Stafford Hospital that leadership sometimes dramatically fails to cope.
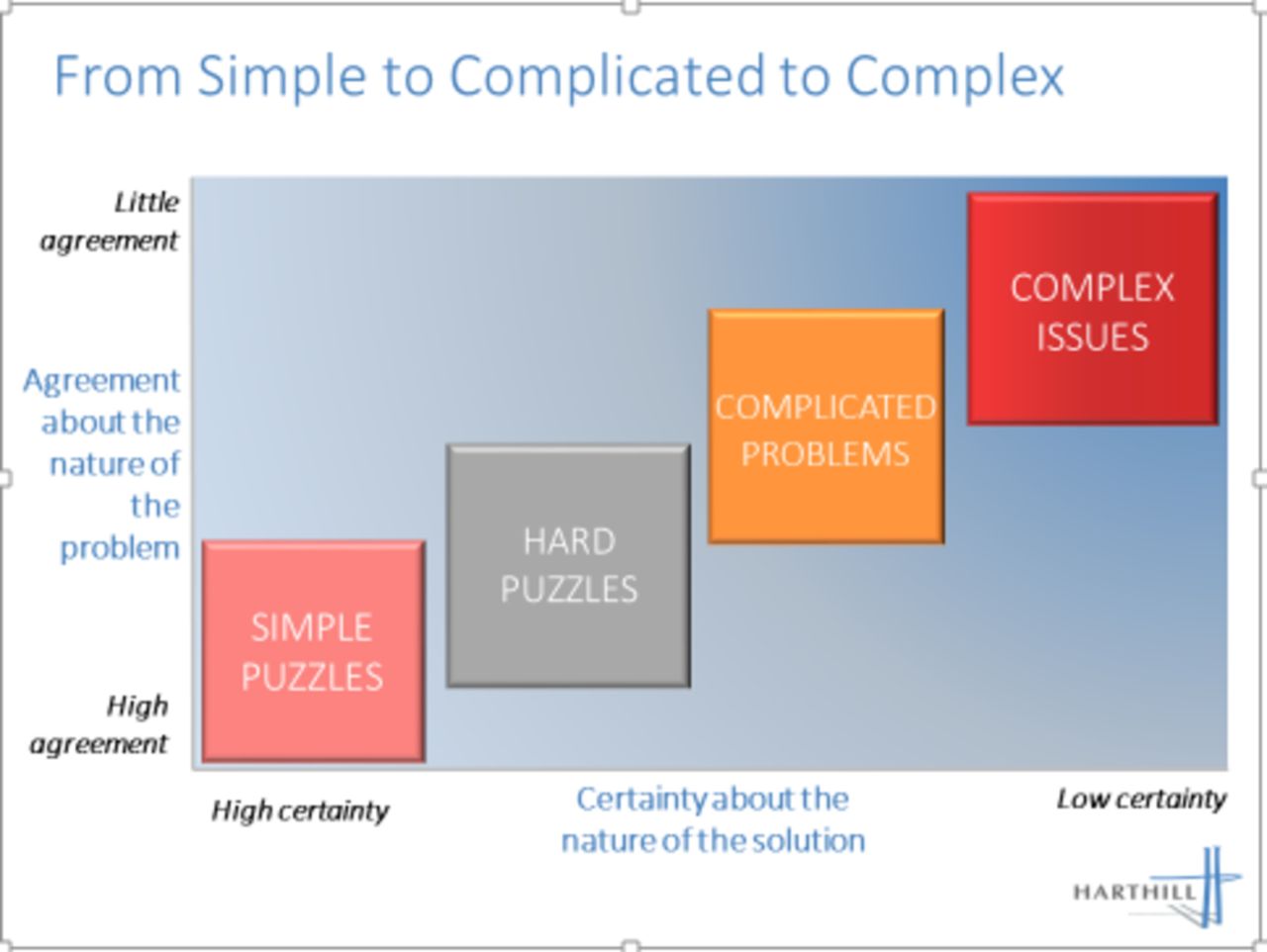
I have found a straightforward model, derived from the work of David Snowden3 extremely useful in considering two aspects of VUCA—complexity and ambiguity (see Figure 1). Each day, leaders face a range of situations and challenges, some of which are relatively simple and can be easily resolved. We barely notice our managerial capacity to deal with these until something goes wrong or their volume overwhelms us. For example, responding to individual corporate emails can be simple enough, but when there are 150 plus each day, the nature of the task changes. Some activities are complicated—they require high levels of technical skill and co-ordination. A renal transplant operation is complicated because the route to an already agreed solution is known—it is within our experience. It may be extremely difficult to accomplish and there may even be an expectation of a certain percentage of failures, but the dimensions are known. Managing the growth and impact of obesity, in contrast, is complex. The causes are multifactorial and there is disagreement about the causes: poverty, social class, sugar, fast foods, TV dinners, inadequate exercise, low self-esteem and corporate greed are all factors named—each giving rise to potentially different management strategies. Consequently, there is little agreement about the best remedies. The UK government’s announcement of a limited tax on sweetened carbonated drinks raised a storm of protest from the drinks industry and those concerned about a nanny state, with simultaneous cries of ‘not enough’ from the medical world.

{kind=link}
The increase in complexity of problems facing leaders.
Leaders need to be able to distinguish the simple from the complicated from the complex and once they have done so must be able to respond appropriately. The education and on-the-job learning process that we expose most medical leaders to, and particularly those who have trained as doctors or nurses, encourages the development of capabilities designed to deal with the complicated, but which are inadequate for the complex. Doctors soon specialise and become highly expert in a particular field. This is, of course, extremely helpful in that disciplines, such as neurosurgery, have developed their craft to deal with unimaginable levels of intricacy to create remarkable outcomes. However, a consultant who day after day works with microscopic detail may not be developing the skills to guide a department or whole hospital through the many complex challenges that it routinely faces.
The NHS in England reportedly deals with over 1 million patients every 36 hours.4 The sheer scale of this creates pressures on leaders and they respond to the perception or reality of overload in a number of ways. As stress rises beyond an optimum point, performance is damaged, but even before this point leaders may confuse the appropriate response to the issues in front of them. Complicated issues require a different response to complex ones. For complicated issues, the solution is likely to be generated by extensive analysis of the issue and by calling on previous experience. This is a domain where expertise has a high value. In a complicated situation, at least one right answer may exist, but in a complex situation, a ‘right answer’ may not exist at all. What is the ‘right answer’ to the situation in Syria? Well it depends on whether you are a member of Isis, the Assad regime, an opposition group, a Russian, American or Iranian politician, or a civilian living in Aleppo. In complex responses, the leader needs to understand as much of the whole field as possible, sensing what may be possible and respond, not with ‘the answer’ but with emergent actions.
And here is the leadership development challenge! Leaders can only develop the capacity to interpret and engage with the wider system in any reliable way by developing their invisible ‘sub-structure’ of meaning making.5 By meaning making, I mean the entirely internal and continuous processes of making sense of our world which drives our actions-in-the-world. This is a capacity that grows and extends with living. The child psychologist Piaget6 noted that children move through progressive sequences of being able to interpret their world, from simple ‘magic’ reasoning towards ‘formal operations’ with the ability to reason abstractly. These are distinctive and progressive stages of meaning making in which each stage contains the sub-structure of the previous stage and goes beyond that logic in a series of ‘include’ and ‘transcend’ steps.
Piaget believed that this stage-wise development ceased with what he called formal operations, achieved some time during adolescence. However, extensive and multisource research since Piaget has identified that we extend the capacity to make meaning in differentiated and ever more complex stages into late adulthood. As we have said previously, the good news is that individuals are able to accumulate wisdom over time by restructuring how they make meaning. The bad news is that this process can and does get arrested or blocked.
The Leadership Development Framework describes this stage-wise development, applying single-word descriptors or labels to each stage. Each meaning-making stage is called an ‘Action Logic’. Harthill has profiled over 5000 leaders working in organisations internationally and has researched the impact of leaders who profile at different Action Logics7 (see table 1 for a brief description of each Action Logic). The vast majority of leaders working in organisations profile at the Achiever Action Logic (55%), while (26%) profile at Individualist. Of critical interest is the number of leaders that profile at the Strategist Action Logic. This is where the rubber hits the road in a VUCA world. It is leaders at the Strategist Action Logic that are significantly more able to successfully deal with complexity and ambiguity. Their processes of meaning making are increasingly inclusive of divergent perspectives, are able to hold opposing ideas in relationship to each other and can assimilate operational paradoxes (such as slowing down to move more quickly) with ease. The consequence of this is the capacity to observe the dynamics of a system more acutely and to choose, with greater wisdom, possible leverage points.
Brief descriptions of key action logics and distribution in a population of 5000 organisational leaders
Yet, only 5% of leaders profile at the Strategist Action Logic. Why? In order to understand this, it may be helpful to follow the development of the imaginary doctor Jane Rodrigues through a number of developmental steps, each one represented by an Action Logic. Jane remembers vividly the transition from studying 10 General Certificate of Secondary Education (GCSE) subjects to a focus on four ‘A’ levels. GCSE lessons provided a usually undemanding place to hang out with a chosen group of friends—in fact, Jane remembers more clearly the importance of being part of her friendship group, with its moving clan membership and the dance around boys, than she does about the particular subjects. This was an adolescent phase when Jane’s dominant Action Logic was Diplomat. Her key orientation was to the social group and her place in it.
In choosing predominantly science subjects for her ‘A’ levels, Jane was already casting an eye to her future—her question was not ‘what are my friends doing’ but ‘what am I good at, what interests me?”. Moving into ‘A’ levels, she felt a different tempo and a different orientation to the subjects—drilling down deeper revealed levels of knowledge that really interested her and she readily absorbed new information. For the first time, she started to enjoy the analytic approach of science and began to think of herself as a scientist-in-the-making. Jane was moving from the Diplomat firmly into the Expert Action Logic.
This move was consolidated as she started her training to be a doctor—drilling down even more deeply into the science of medicine and identifying herself as a scientist and as a doctor-in-the-making. She also remembers some challenges to the otherwise enjoyable linearity of this development. In an optional module, the anthropology of medicine, she was confronted with the importance of culture, belief and myth in shaping how medicine is used and how effective it is. She discovered that identical drugs or procedures sometimes have radically different impacts in different parts of the world.
A part of her awareness was troubled by this, but the operating norm all around her was that, through analysis, we can discover the one truth, so she parked this and continued with the demanding process of learning both facts and clinical practice. However, a seed was sown that would germinate later.
Through her junior doctor years and then into her first specialism, in burns and plastic surgery, she developed highly focused specialist skills—reinforcing the Expert Action Logic. Her work in the burns unit became increasingly rewarding as her ability to complete complex procedures grew.
As a consultant, she started to learn the absolute necessity of personal efficiency as the demands on her were greater than the time available. It seemed to her that the biggest challenges lay not in her technical skills but in getting through the seemingly impossible list of what needed to be done each day. Stamina was the order of the day, and so was ruthless efficiency. She managed herself, and she started to be aware of the action, or inactions, of others. She became aware that she was working within a system and that no matter how personally effective she was, the system itself could be confounding. Jane was extending her Expert Action Logic by adding the perspectives and constructs of the Achiever Action Logic.
In the next 12 years, Jane worked in five different hospitals. The impact of the culture and efficiency of each hospital made a noticeable difference to patient outcomes and Jane’s attention moved beyond developing her own technical skills to the tricky question of organising. As she became a medical lead, she became a competent people manager, noticing the connection between the morale of staff and patient outcomes. She became curious about what impact she might have and consciously experimented with different styles of influencing meetings, sometime advocating a position strongly and sometimes holding back her opinion and summarising the key points. She attended some leadership courses and learnt her Myers Briggs type. In this period, Jane was extending the Achiever Action Logic to include the next stage, the Individualist Action Logic.
In her forties, Jane made a significant move—to what some colleagues call ‘the dark side’—and she took on a clinical director’s role that saw her time in the ward and theatre reduced. She encountered the full force of leading in a VUCA medical world. On the one hand, she was required to reduce her budget by 4% each year, while experiencing a steady rise in patient demands, particularly in alcohol-related and knife-related injuries. There were staffing shortages in key areas that seemed impossible to resolve without engaging agency staff and wrecking the carefully generated savings. In addition, she took on a lead role in hospital-wide patient liaison. She now needed to lead in an expanded context—within an organisational system that reached out beyond her department, beyond the hospital to the NHS Foundation, the Clinical Commisioning Group (CCG), local and national politicians, the police and social services, pharma companies and the local community. Managing her most scarce resource—time—Jane started to see her role as catalytic. She sought leverage points and sources of energy in the system to encourage, connect to each other and to support. She became deeply curious about how to create positive movement in such a complex system. In this time, Jane started to extend her Individualist Action Logic to include Strategist. She was moving into the one in 20 leaders in large organisations that make meaning from this perspective.
Leaders who can access the Strategist Action Logic often make a profound impact on the organisations8 within which they work, and Harthill has researched and observed these leaders in action. We have identified that there are six key capabilities common to these leaders and vital to the way they operate within their organisations. Each capability is explained briefly and illustrated by how Jane used this in her leadership.8
Inquiry-based experimentation weaves together inquiry, action, experimentation and learning. It requires the leader to practice, at least temporarily ‘not-knowing’ and so to inquire of themselves, their colleagues and the system. As Jane’s confidence grew, she was more able and willing to inquire—seeking the perspectives of colleagues rather than advocating her own position. By inquiring, she saw new angles on problems, which enabled her to trying doing some things differently, to be experimental. Her experiments were carried out consciously and Jane became an innovator—someone who would question old orthodoxies and find new routes forward by trying new approaches.
Dancing between vision and detail involves leaders in simultaneously holding a sense of direction (something they stand for or believe in) and being able to dive into the detail through which reality becomes manifest. This ‘dance’ was a challenge for Jane because her comfort zone had always been in the detail, and she had to discipline herself to stand back more, to delegate and choose when to dive in. She discovered that it is the fluidity of this movement which is important—being able to get involved in the detail and then pull back to use the detail to inform a wider perspective.
Perhaps more than any other single capability, Jane embraced the paradox of passionate detachment. No one doubted her passion for the patients—this had led to her driving herself hard and, in turn, driving others hard. There had been times when her stress levels were dysfunctionally high and home life rocky. A coach had helped her to step back, to develop personal techniques to be less wound up such as literally pausing for breath. Jane found she could do this without caring one jot less—this ability to not get sucked-in enable her to be more strategic in her leadership. Jane noticed that remaining calm and centred reduced frustration and enabled better decision-making.
The courageous use of power started with Jane consciously recognising the power, both formal and informal, institutional and personal, that she held. She noticed, for example, how people deferred to her as a consultant surgeon and the effort required to actively resist this in order to involve others. Unlike some of her colleagues, she sought out more mutuality and less deference to the ‘natural’ hierarchy. Jane also recognised that her courage was sometimes required to resist what she thought was muddle headed or immoral, or to bring new thinking to the table. She increasingly found herself speaking truth to authority in uncomfortable situations.
The positive use of language requires leaders to attend to two aspects of what they say. First, it is through language (including body language and the written word) that leaders communicate their hopes, desires and fears. Jane learnt that no matter how tough the current situation might be, it is her role to communicate her belief in a better future, while being honest about the difficulties of the present moment. Jane also learnt that she needed to consciously structure what she wanted to say, ensuring a skilful blend of advocacy and inquiry.
The final key capability, exercising systems leadership, grew steadily in Jane as the demands on her to work in ever larger parts of the system expanded. She remembers the day when angry about some administrative nonsense that pinned her staff down on redundant data generation; she calmly reviewed where the demand was coming from, who the stakeholders were and what could be done to reduce the burden. Despite the initial resistance of some colleagues, she was able to reduce the management information significantly, with no obvious negative impact.
Jane through a mixture of experience and learning had included the Strategist Action Logic in her meaning-making capacities. Leaders work in increasing complex and ambiguous contexts—and to help them be more effective they will do well to move developmentally towards the Strategist Action Logic. What advice do we give leaders in order to help with this movement?
First, no matter what your age, take the possibility of your development, of becoming a wiser and more capable leader seriously. We say this because development cannot be taken for granted—experience is not a teacher per se, a process of reflection and learning is required in order to convert experience into wisdom. Make your experience a source of learning—by developing effective reflection skills and techniques and top this up by attending courses that will increase your self-knowledge.
Second, expose yourself to different experiences—try different roles, volunteer for different task groups, question your habits of mind and behaviour be open to what might emerge. In a word—be curious.
Third, look around for inspiring role models. Although only 5% of leaders profile at Strategist, you will probably know one and be able to observe how he or she works. You may not know if they are Strategists, nevertheless identify leaders that make a significant contribution, work in unconventional ways sometimes, have their finger on the pulse and seem surprisingly well networked. Learn by observation and, if possible, questioning.
Footnotes
Contributors DR: Research by Harthill Consulting Ltd.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.