Article Text

Abstract
Background Previous embedded researcher models have focused predominantly on an individual being a temporary team member and embedded for a project-limited short-term placement.
Aim To develop an innovative research capacity building model to address the challenges of developing, embedding and sustaining, research led by Nurses, Midwives, and Allied Health Professionals (NMAHPs) in complex clinical environments. This healthcare and academic research partnership model offers an opportunity to support the ‘how’ of enabling NMAHP research capacity building from within the researchers’ clinical area of expertise.
Method Collaboration between three healthcare and academic organisations and the iterative process of cocreation, development and refinement took place over 6 months during 2021. The collaboration relied on virtual meetings, emails, telephone calls and document review.
Results A codesigned NMAHP embedded research (ER) model is ready for trialling with the individual being an existing clinician working collaboratively within the healthcare setting and with academia to develop the skills to become the ER.
Conclusion This model supports NMAHP-led research activity in clinical organisations in a visible and manageable way. As a shared, long-term vision, the model will contribute to research capacity and capability of the wider healthcare workforce. It will lead, facilitate and support research in and across clinical organisations in collaboration with higher education institutions.
- research
- capability
- capacity
- career development
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Academy of Medical Sciences1 advocates collaborative working across all professions and sectors of the ecosystem to accelerate the translation of research for patient benefit. However, the research infrastructure to facilitate this vision has been hampered by many challenges. At micro-systems level, nurse, midwife and allied health professional (NMAHP) practitioners must balance complex clinical roles with academic development amidst staffing shortages and increasingly challenging contexts. At mesolevel and macrolevel, the challenge for policy-makers and leaders is how to create a system infrastructure which enables the workforce to keep pace with the innovations needed in clinical practice. The additional challenges of accessing expert leadership, support and mentorship, optimising career progression and reaching a satisfactory balance between clinical and academic development which achieves all four pillars of practice (clinical, leadership, education and research) make impactful collaborations difficult to accomplish.2 It seems that regardless of the commitment to embedding research activity, the reality is challenging.
Sustained knowledge translation into practice requires expertise in developing contextual readiness.3 4 The use of best evidence to support practice and the generation of new knowledge to use in practice are the hallmarks of excellence.5 Established embedded researcher models are predominantly based on an individual being a temporary team member, embedded for a project-limited short-term placement. This may not readily enable the longitudinal translation of improvements into practice, potentially due to a lack of connection between the producers and consumers of evidence.6
The continuation of research activity and the recognition of experience and expertise following completion of an academic programme are often reported to be unsupported and undervalued in clinical practice for NMAHPs.7 8 While work has been undertaken to develop advanced practice roles,2 limited job opportunities and few developed career pathways located in clinical organisations which truly support the research pillar of practice exist.
The embedded researcher (ER) model proposed here is designed to build on established ER models. This may achieve a threefold benefit. The first relates to the research capacity building of NMAHPs; the second is the potential to address the perceived gap between evidence production and consumption in clinical settings; and the third supports greater collaboration between academia and healthcare.1 9–11 Its intention is to support registered NMAHP staff to become the ER in their practice environment, at the same time enabling the organisation to better articulate its key priorities via an applied research focus.
Embedding research, as part of evidence-based practice to make sustainable improvements that are transformational, requires
Executive and departmental leaders who commit to core funding for research focused roles or agreement for dedicated research time within existing/future NMAHP job roles on a permanent basis.
A commitment to collaboration through formal clinical–academic partnerships in which all partner organisations recognise and value opportunities that enable authentic collaboration, knowledge-rich organisational and research evidence which informs decision-making and integrated skill sets.
A focus on research important to the local population.12
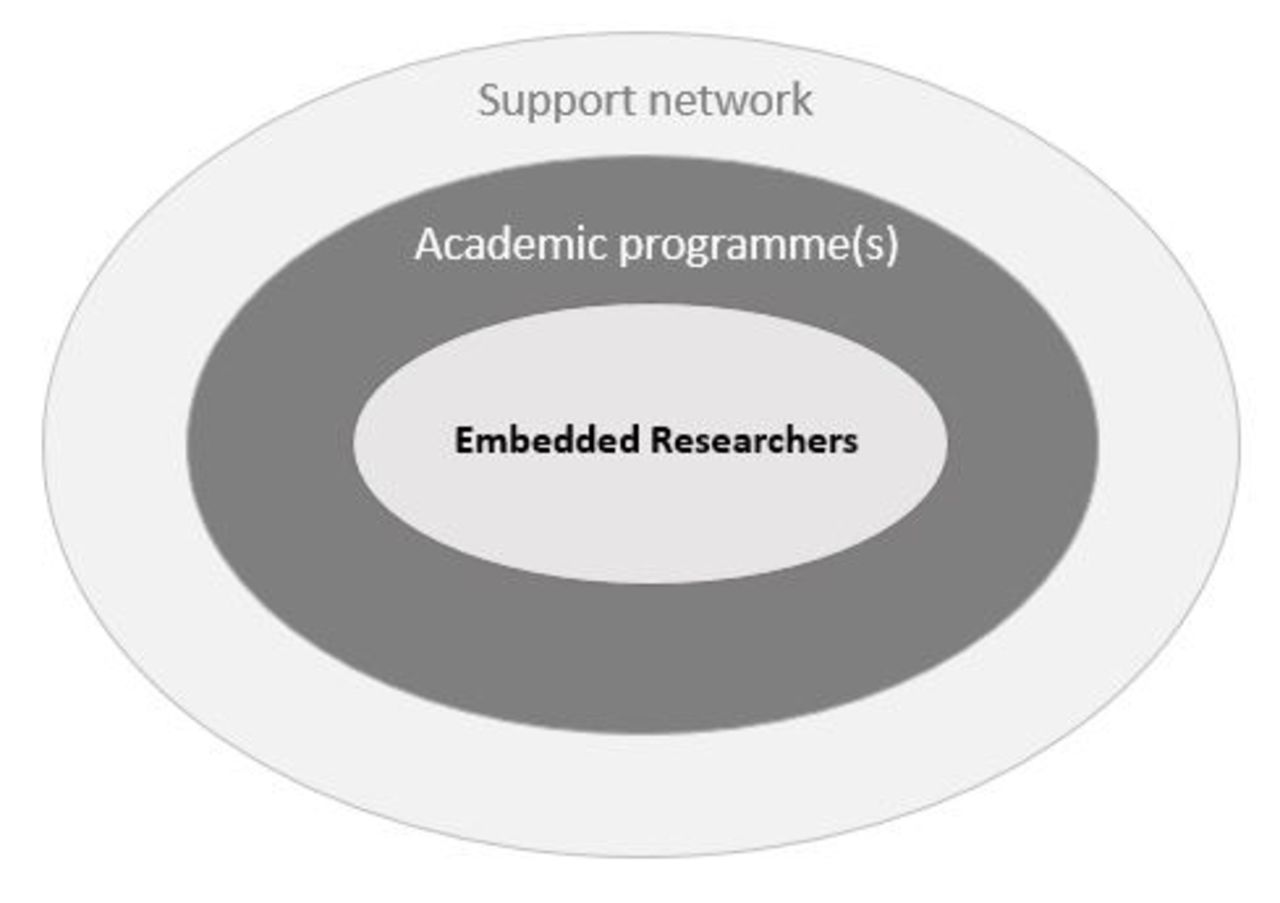
To meet these challenges, an NMAHP-ER model (figure 1) was codesigned between the James Paget University Hospitals NHS Foundation Trust (JPUH), The Newcastle upon Tyne Hospitals NHS Foundation Trust (NuTH) and the University of East Anglia ImpACT Research Group. To become truly embedded, we propose a value-based approach built on interprofessional learning to achieve the transformation of and review the impact of NMAHP led research activity.13 The key foundation of the role has the individual clinician working collaboratively within the healthcare setting and in partnership with academia to develop the skills to become the ER. The model will be trialled across two NHS settings in England (JPUH and NuTH) differing in size, context and research infrastructure.

{kind=link}
The NMAHP ER Model components.
To evaluate the impact of the ER model, we propose a realist evaluation approach to identify the mechanisms that work and do not work, for whom, in which contexts and why.14 The evaluation will also explore the learning processes and impacts of the overarching programme, for career pathway development for ERs. The evaluation observations will contribute to the development of an implementation and impact framework which will seek to sustain the transformations achieved by the initiative in practice going forwards. This framework will identify the micro, meso and macro enablers, and activities that need to be in place for organisations to invest in for the future. It will enable recommendations to be made to commissioners, funders and policy-makers regarding the growth and sustainability of this vital workforce if the NHS is to transform and keep pace with the increasing complexity of the challenges it faces.
Model development
An iterative process of cocreation and refinement took place over 6 months during 2021. The development of the NMAHP-ER model was informed by dialogue from tweet chats, scoping of existing literature on ER models and shared reflections. Such reflections included collective experiences and the challenges of building research capacity and capability in the NMAHP workforce across stakeholders. The collaboration relied on virtual meetings, emails, telephone calls and document review.
There are many ER approaches across the UK, often reporting limited utility and impact of academic research, a desire for better situated and ‘useful’ knowledge to help them address service delivery issues and a desire for closer interactions with researchers.4 15 Our NMAHP-ER model has cocreated an approach to embedded research that will meet the needs of our organisations with the learning and evaluation explicitly built in. This enables participants to develop the essential skills required to embed research outcomes and subsequent change across services, organisations and systems. The NMAHP-ER model is unique because it is clinically led incorporating support with the wide range of skills (particularly linked to quality, safety and effectiveness) that enable insights resulting from research in and from practice to be implemented and sustained and with evaluation which embraces changes in practice and policy.
The embedded researcher model
With NMAHP-ERs at the centre, the model is reinforced by a support network and academic development through research training, while being underpinned by the components of the venus model of person-centred sustainable transformation.16
The ER
The process for identifying and appointing into the ER role will purposefully account for the contextual differences and ‘readiness’ of departments to embrace the role across the pilot sites. The detail of that process will therefore vary between organisations, however, it may include an NMAHP clinician being allocated dedicated research time within their existing contract as part of core service funding or appointing to a new post through grant income or other internal/external funding streams where appropriate.
An ER working within clinical teams enables the generation of potential research and evaluation questions alongside colleagues and patients. The eventual topic under study thus becomes one which has been coproduced, aligning closely with the broader strategic aims of the department and key stakeholders. Embedded research and academic activity occur as integral to and informing the ER’s clinical role, serving to role-model the ER as visible and alongside colleagues in the clinical areas.
The support network
Our ER model enables practitioners to work directly with the audit, research, quality improvement and/or service evaluation teams in the hospital, alongside departmental/directorate links depending on the focus of their project(s). They may also link to a ‘site-specific’ employee or a patient/volunteer working with the organisation (or combination), who has specific focus or interest in the area. A three way critical companionship connects the ER, a trust executive and non-executive director (NED), enabling mutual and reciprocal learning and addressing executive buy-in as a key to success. This will directly connect the ER to the trust board throughout the pilot phase of the model for the purpose of learning what works. For example, an ER based in a maternity service in an area of deprivation may link to the Maternity Voices Partnership group (a team of pregnant people, service users their families that are experts by experience, working in collaboration with commissioners) as ‘site specific’, and attend bimonthly meetings with NED/Executive maternity links.
Academic development and career progression
An academic mentor links to each ER as part of the Professorial Network at the Higher Education Institution (HEI). Through local reciprocal arrangements, the mentor provides academic and career advice and acts as a critical companion.
To build their research knowledge and skills, ERs will undertake a programme of study at either masters or doctoral level as part of their appointment. Appointment onto the ER model will be timed appropriately in order to enable 6–9 months ‘lead-in’ for cocreation of research priorities and the question to be explored, completion of a masters’ or doctoral programme and 6 months dissemination, implementation and consolidation time. Application to academic programmes is undertaken during the lead-in time (the first 6 months) and programmes may be funded through continuing professional development monies, external grants, charities or other appropriate routes supported through the organisation. Funding for the academic programme should be considered as integral to the role prior to any ER appointments.
The team approach to codesigning research priorities and the question to be answered is key to the overarching aims of the pilot and therefore its success. With this in mind, to maximise the value of the whole research process and the learning potential across the whole pathway, individuals appointed to new posts would not have already commenced a masters or doctoral pathway.
Integral to this model is a commitment through the clinical and academic organisations to job-plan research activity into the individuals’ onward career pathway. This may include (but not be limited to) routes such as joint clinical academic practitioners, multiprofessional consultant practitioners and advanced clinical practice. The career development pathway is underpinned by a programme of workplace learning to enable the ER workforce to develop the capacity and capability for clinically led research and transformation underpinned by the venus model.14
The venus model
The venus model,14 informed by a decade of applied research on workforce and systems transformation, aims to use the workplace as the main resource for learning. It identifies five integrated skill sets of facilitation, innovation and improvement, practice development, culture change and leadership as central to achieving effective, sustainable change across health and care systems by focusing on what matters most to people (patients, citizens and staff) in partnership. These five core skill sets intertwined with the research capacity building activities provided through the ER model are the cornerstone of the development of ERs as research leaders.
Discussion
NMAHPs are perfectly positioned to innovate, discover and implement improvement activity through research in and from practice17 aligned to what matters to people in complex contexts. They are strategic, able to generate income, key to forging progress in building capacity and capability of the workforce and drive research for patient and staff benefit. Engagement in research activity can positively impact morale and job satisfaction in staff.18
The importance of having dedicated leadership to drive forward and support implementation of the model in its entirety may be quite radical for some and could present a potential limiting factor to the success of the NMAHP-ER model. The model may require organisations to adopt a pump-priming approach to realise the benefits of these roles. This may be possible through initial funding of a new post or providing dedicated research time to existing posts through core/establishment funding. When considering ‘return on investment’, organisations and/or departments will need to be clear of their own definition of ‘value added’ when evaluating or measuring the success or outputs of these roles. For example, value may be attributed to patient experience, patient outcomes, workforce recruitment, retention and productivity and financial, social, environmental, green healthcare and well-being factors or a combination of all or some of these.
Our model requires long-term vision and planning to build NMHAP inclusive research cultures, leaders and expertise. For those in decision-making positions within the clinical environment, whether they possess the real-world research readiness within their own armoury or not, whole system collaboration fueled by a ‘leap of faith’, drawing on the full potential of the workforce and its expertise to benefit quality care and services, are the foundations to making this happen.
Conclusion
As a cocreative model, the NMAHP-ER model holds significant potential to generate and sustain NMAHP-led research activity in a range of clinical settings regardless of context. The model is a pragmatic mechanism enabling embedded NMAHP research whose design is whole organisation and system friendly, being highly visible, realistic and manageable. The imminent testing phase will identify the longevity of its sustainability. As a collaboration between clinical and academic partners, it can directly contribute to the building of long-term capacity and capability in the wider healthcare workforce, through supporting, facilitating and leading research.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank Kirsty Cater, Rene Grey, Paul Charlton and Ian Joy for critical review of the model in the clinical practice context and contribution to intellectual content of the manuscript.
Footnotes
CLW and LT are joint first authors.
Twitter @ClaireW_UK, @TinkleLin, @IPDKim
CLW and LT contributed equally.
Contributors CLW and LT: original concept generation and substantial intellectual contribution to model design and development, leading work in practice, development and leadership in manuscript writing and responsible for the overall content as guarantors. CJ and HH: substantial contributions to the design and development of the work and intellectual content of the manuscript. JC, PM, JW, SH and KM: intellectual contribution to development of the work and drafting and revision of manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests CLW and LT are National Institute for Health Research (NIHR) '70@70' senior nurse and midwife research leaders. The views expressed in this article are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Provenance and peer review Not commissioned; externally peer reviewed.