Article Text

Abstract
The lack of both women and physicians from groups under-represented in medicine (UIM) in leadership has become a growing concern in healthcare. Despite increasing recognition that diversity in physician leadership can lead to reduced health disparities, improved population health and increased innovation and creativity in organisations, progress toward this goal is slow. One strategy for increasing the number of women and UIM physician leaders has been to create professional development opportunities that include leadership training on equity, diversity and inclusivity (EDI). However, the extent to which these concepts are explored in physician leadership programming is not known. It is also not clear whether this EDI content challenges structural barriers that perpetuate the status quo of white male leadership. To explore these issues, we conducted an environmental scan by adapting Arksey and O’Malley’s scoping review methodology to centre on three questions: How is EDI currently presented in physician leadership programming? How have these programmes been evaluated in the peer-reviewed literature? How is EDI presented and discussed by the wider medical community? We scanned institutional websites for physician leadership programmes, analysed peer-reviewed literature and examined material from medical education conferences. Our findings indicate that despite an apparent increase in the discussion of EDI concepts in the medical community, current physician leadership programming is built on theories that fail to move beyond race and gender as explanatory factors for a lack of diversity in physician leadership. To address inequity, physician leadership curricula should aim to equip physicians to identify and address the structural factors that perpetuate disparities.
- medical leadership
- career development
- career
- clinical leadership
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The principles of equity, diversity and inclusion (EDI) have been endorsed formally and symbolically for several centuries in the USA and Canada.1–3 However, they have coexisted with enormous discrepancies rooted in systematic exclusion and with ongoing debate about how these principles should be enacted.4–9 Most recently, these issues have gained renewed prominence through the #MeToo, #UsToo and Black Lives Matter movements, which have affected nearly every sphere of North American society, including healthcare.
In this context, the persistent lack of women and under-represented in medicine (UIM) physicians in leadership remains a concern in healthcare. Studies have shown that reducing health disparities and improving healthcare outcomes of diverse populations require more diversity in medical leadership.10–14 It is also well established that diverse and inclusive workplaces benefit everyone.15–17 When diverse groups come together to resolve a problem, the power of collective intelligence creates better solutions.18 People with different assumptions and experiences can question norms and provide perspectives that are not possible with less diverse groups.19–21 The range of ideas that diverse groups bring can be immensely generative. This instrumentalist argument has been used to promote diversifying physician leadership. Medical organisations and most faculties of medicine in North America are developing frameworks for equity and inclusion to realise the benefits of a diverse medical workforce for patients, faculty and the institutions themselves.
However, while institutional leaders have been claiming for more than a decade to be recruiting and retaining a more diverse physician workforce, progress remains slow and inequitable.22 Several studies have shown that women and UIM physicians still lag behind white male physicians, not only in terms of being represented relative to their numbers in the general population,23 24 but also in terms of leadership positions, first-authored publications, research funding, performance evaluations, awards, promotions and salary.25–33 Various factors underlie this lag, including lack of mentorship, fewer resources (eg, personnel, space, equipment) and less award recognition.25–27 34–36
One of the principal strategies for increasing the number of women and UIM physicians in academic medical leadership has been to create professional development opportunities. However, it is not clear whether these leadership programmes can change the culture of white male leadership in medicine. It is not even known to what extent concepts related to EDI are included in this programming. In this paper, we performed an environmental scan to explore three questions: how physician leadership programmes address EDI in their curricula, how they are evaluated and how EDI is being discussed in medical education.
Methods
Since there is no consensus on how to conduct an environmental scan,37 we modified Arksey and O’Malley’s38 scoping review framework for the purposes of mapping the available evidence and identifying/analysing knowledge gaps. The scoping review approach to gathering information was helpful because it provided a systematic process for data gathering. Our environmental scan moves beyond the purpose of a scoping review which is to provide a broad survey of the literature without necessarily including programmatic recommendations. We offer a way forward to help programme directors consider the future direction of their physician leadership offerings.
Our environmental scan was completed in July 2020. We chose not to search for articles beyond that date for two reasons. First, most physician leadership programmes were cancelled during the first wave of the COVID-19 pandemic and most research studies pivoted to issues specifically related to the pandemic. Second, the summer of 2020 marked a profound shift in perceptions about race across North America due to the strength of the Black Lives Matter Movement. Due to some limitations with resourcing, we were unable to quickly reconceptualise how this shift may have altered physician leadership programmes, particularly as they were simultaneously impacted by the pandemic and increasing digitisation. We anticipate that future studies may uncover more nuanced approaches to physician leadership that take these shifts into account; however, this scan offers a ‘snapshot’ of activities up to these significant shifts in the summer of 2020.
To create boundaries around the environmental scan, we focused on continuing professional development related to physician leadership and excluded any leadership initiatives for undergraduate or postgraduate medical trainees.
Stage 1: identifying the research questions
We developed three research questions: (1) To what extent is EDI-related programming present in physician leadership programmes currently offered in Canada and the USA? To answer this question, we searched the grey literature for physician leadership programmes in North America. (2) What are the reported outcomes of physician leadership programmes, particularly those related to EDI in the peer-reviewed literature? To answer this question, we searched the peer-reviewed literature. (3) How often has EDI been broadly discussed in the medical education community in the past 5 years? To answer this question, we searched selected Canadian, USA and international medical education conferences for EDI content.
Stage 2: identifying relevant studies
Physician leadership programs
Grey literature is information that is produced outside of traditional publishing and dissemination channels (ie, government documents, brochures, conference proceedings). When searching the grey literature, there is no ‘one size fits all’ approach,39 although searches should be replicable and drawn from the most up-to-date sources.40 Searches also need a boundary or ‘end point’ to ensure they are both useful and feasible. To ensure that our search was feasible, we only searched the top 12 ranked schools and the separate list of organisations. While we recognise the limitations of using reputational surveys or university rankings,41 42 we purposely selected top-ranking schools because they are perceived as leaders and have greater access to resources and funding. It is reasonable to expect that perceived leaders would and should attempt to set the standard for forward-thinking EDI physician leadership programming although we recognise this may not be the case.
To identify physician leadership programmes, the librarian (RB) compiled a list of the highest-ranking medical schools in Canada and the USA. Schools were identified through Maclean’s Rankings of Canada’s Best Medical Doctoral Universities43 and the Wall Street Journal/Times Higher Education Rankings.44 In our list of top five schools in Canada and the USA, there was a tie for fifth place in both countries. This meant that 12 medical schools were included in our scan. RB also compiled a further list of resources (eg, medical associations, professional organisations). Removing duplicates produced an additional list of 21 web links to potential leadership programme webpages that were added to the initial phase of the search. Part of the search process included looking for programmes, courses and seminars targeted towards physicians with keywords such as Leadership, Leading, Leader and/or Diversity, Multicultural, Women, Minority and other related terms in the programme titles.
Peer-reviewed literature
RB developed a comprehensive international search strategy to explore the Medline, Embase, Web of Science and Scopus databases for articles published since 2013. We chose 2013 because a previous systematic review of physician leadership programmes included results up to that year.45 The search of peer-reviewed literature included controlled vocabulary in the form of database-specific subject headings, as well as relevant free-text keywords. Search terms included physicians in hospital, medical or healthcare environments; leadership development programmes; and diversity criteria. The searches were conducted in July 2020, and initially no language limits were applied. The full Medline search strategy is available in online supplemental appendix A.
Supplemental material
Conferences
A search of international physician association websites was conducted to locate relevant conferences held between 2016 and 2020. We compiled a list of organisations that held the most visible and well-attended medical conferences to explore how EDI concepts have been discussed in the medical community. We scanned conference brochures, agendas and website materials, screening titles and summaries of conference events to explore programming in relation to EDI, race and gender. If conference material was unavailable online, GB requested a copy. The scan criteria were not limited to specific physician leadership content but rather sought to explore EDI teaching at these conferences more broadly.
Stage 3: study selection
Table 1 summarises the individual inclusion and exclusion criteria for physician leadership programmes, peer-reviewed literature and conferences.
Scan inclusion and exclusion criteria
Stage 4: charting the data
We developed three data abstraction forms, one for each research question. SS, BL and GB drafted the forms which were further refined by all remaining authors. SS and BL completed the data abstractions and discussed any conflicts until consensus was reached. Online supplemental appendix B provides detail on the specific categories included in the data abstraction form.
Supplemental material
Stage 5: collating, summarising and reporting the results
Physician leadership programs
After the inclusion and exclusion criteria were applied, 35 programmes were identified for a full review. We found that 16 (46%) programmes had 1 or more references to EDI, gender or race in their website information or programme agenda. Of the 16 programmes that referenced EDI, 8 were categorised as general leadership programmes, meaning they were open to all physicians.46–53 Six programmes were designed for women,54–59 and two programmes were designed for UIM physicians.60 61
Peer-reviewed articles
The initial search of peer-reviewed articles yielded 4887 studies (4857 studies from database search, 30 studies identified through additional sources), of which 980 duplicates were removed (see figure 1). SS completed title and abstract screening on the remaining 3907 studies using the inclusion/exclusion criteria. Seventy-nine studies were assessed as eligible for full text review. SS and BL assessed those studies and identified 19 studies that included an evaluation of their physician leadership training programme. Of the 19 physician leadership studies, 8 were offered for all physicians.62–69 Nine studies focused on women physicians70–78 and two studies focused on UIM physicians.79 80
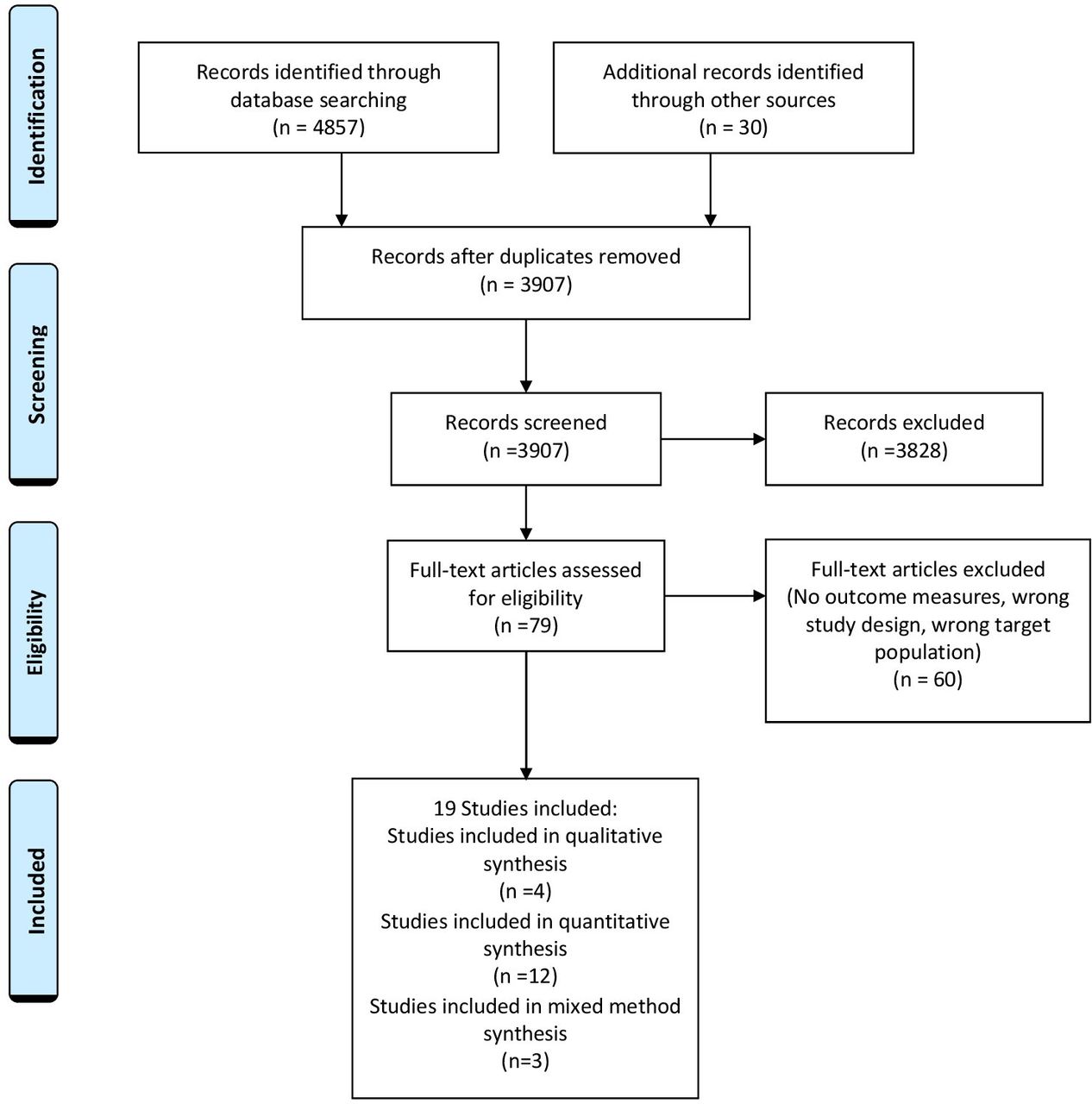
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of study selection.
Conferences
After accounting for cancelled conference events and conferences that had not been running for the full 5-year period captured in our search (2016–2020), 7 conferences, which equated to 30 individual conference events, were included in our review.81–110
Results
Physician leadership programs: to what extent is EDI-related programming present in physician leadership programmes currently offered in Canada and the USA?
Programme characteristics
Of the 16 identified programmes, 4 were from Canada and 12 were from the USA (see table 2). For ease of reference in our discussion, we refer to all initiatives as programmes.
Characteristics of physician leadership programmes
EDI programming: general leadership programs
Of the eight general programmes identified, five programmes had at least one learning objective or desired outcome that related to EDI.46 48–51 Seven programmes contained curriculum items (eg, a module or workshop) that addressed EDI, gender or race within the context of leadership.46–48 50–53 One programme contained a module about systemic racism and equity within primary care.48 Only one programme, the Association of American Medical Colleges Healthcare Executive Diversity and Inclusion Certificate Programme,46 focused specifically on EDI in leadership. Designed to develop leaders who use diversity as a driver for institutional excellence in practice, this programme featured six modules in which learners design and implement a strategic diversity project in their own institution.
EDI programming: leadership programmes for women and UIM physicians
Of the leadership programmes identified that contained EDI content, six were designed for women in medicine.54–59 Two programmes were designed for UIM physicians.60 61 Programmes were tailored to specific career stages: two focused on early-career physicians55 60; two targeted mid-career physicians56 61; one was for senior physicians aspiring to executive leadership57; and the remaining three were open to physicians at any stage of their career.54 58 59 There were no programmes which specifically targeted physicians who experience multiple types of oppression, for example, women who were members of racialised groups.
The various curricula covered topics common to most leadership programmes, such as negotiation, developing leadership styles, financial management and networking, but explored these topics through the lens of women and UIM physicians. One programme offered a session on time management for women leaders58 and two programmes held sessions on negotiating compensation as a woman.56 58 Two programmes offered sessions on developing a culture of equity, specifically in relation to women in the workplace.58 59 For example, Harvard University’s Career Advancement and Leadership Skills for Women in Healthcare programme58 contained curricula about building strategies to advance women and UIM faculty within academic medicine.
Our review identified two programmes for UIM physicians.60 61 One programme offered a session for early-career physicians on ways to identify and capitalise on leadership opportunities in a climate where UIM faculty are often overlooked.60 The majority of curriculum items focused solely on how UIM physicians navigate barriers within academic medicine, as opposed to sessions which might explore how their identity as a UIM physician may interact with other axis of oppression. However, the second programme for mid-career physicians described a session on identifying pathways to promotion while balancing specific service activities and demands which represent a particular challenge for both women and UIM faculty.61
Peer-reviewed literature: what are the reported outcomes of physician leadership programs, particularly those related to EDI?
General physician leadership programmes
Characteristics of the eight studies (covering seven general leadership programmes) are shown in table 3.
Characteristics of peer-reviewed literature (general programmes)
Physician leadership programs for women and UIM physicians
The remaining 11 studies focused on women and UIM physician leadership (see table 4). Nine studies described programmes for women70–78 and two studies described programmes for UIM physicians.79 80
Characteristics of peer-reviewed literature (programmes specific to women and UIM physicians)
Reported outcomes
Although all of the studies provided robust descriptions of the factors that impede women and UIM physicians in advancing to academic leadership, none provided a theoretical framework for understanding inequity in leadership. Only one study gave an empirical definition of gender inequity; addressed sexual harassment; described the promotion a gender-friendly climate and; discussed the creation of equity policies in curriculum.75 No studies described programme modules, events or training related to race, ethnicity or racism. In terms of models and frameworks that guide evaluation, three studies used Kirkpatrick’s model111 for programme evaluation73 76 77 and four studies chose indicators that were direct measures of the programme objectives.70–72 80 One study used a conceptual model for the professional development of women in academic medicine.74 The remaining three studies did not specify an evaluation framework.
Seven studies reported observable outcomes, including promotion, academic productivity and attainment of leadership positions.70–72 76–78 80 The most robust evaluations of whether physician leadership programmes reduce inequities for women and other UIM groups come from two U.S. studies.71 80 These studies compared programme participants with non-participants and addressed potential covariates. Chang et al’s71 study found that women programme participants were three times more likely than women non-participants to be promoted. However, when women programme participants were compared with men non-participants, promotion rates at 10 years post programme were similar. But because women in general started at lower rates of promotion than men, a similar rate at the 10-year mark merely indicates that the gender gap is maintained, not reduced. This finding suggests that the leadership programme alone was not enough to reduce gender disparities. Guevara et al 80 found no significant differences between the scholar and non-scholar groups in academic promotion or productivity, but they did reveal significant differences in attaining leadership positions. They suggested that the non-significant findings were consistent with the fact that both groups, having negotiated an extremely competitive eligibility process, were already highly competent and that the programme’s success lay in its leadership opportunities not in skills training.
Other studies providing qualitative or anecdotal accounts suggested that leadership training increased career satisfaction70 75; however, leadership programmes alone were inadequate in addressing factors in a large academic and social system that hinder women’s career development.74
Although self-reported satisfaction rates for all of the programmes in this review were mostly favourable, most studies recognised that beyond anecdotal evidence, they could not establish a connection between programme participation and increased recruitment, retention, or promotion. The need to measure other outcomes or to use different evaluation measures, particularly of long-term outcomes, was also identified.62 67 72 73 79 Another limitation was the lack of continued monitoring to understand how the impact on specific subgroups might change as leadership programmes grow.62
Medical education conferences: how often has EDI been broadly discussed in the medical education community in the past 5 years?
Frequency and proportion of EDI, race and gender content in conference material
Overall, the proportion of conference content that focused on EDI, race, or gender was low. Of 1408 keynote, plenary and workshop descriptors scanned, 99 (7%) contained terms that met criteria for inclusion. There was a marked increase in EDI, race and gender conference content between 2018 and 2019: in 2019, 17% of keynotes, plenaries and workshops included EDI, race, or gender content compared with only 4% in 2018. Following this peak in 2019, EDI, race and gender conference context decreased to 13% in 2020. The emergence of the COVID-19 pandemic may explain this decrease: scheduled conferences were either cancelled or pivoted to a virtual format with condensed or refocused programming.
EDI, race and gender terminology
In addition to calculating the frequency of EDI, gender and race related content in conferences, we also explored terminology used in conference titles/descriptors. Binary coding (ie, present/not present), was applied to session titles and descriptors for key terms related to EDI (eg, ‘bias’, ‘culture’, ‘diversity’, ‘equity’, ‘inclusivity’, ‘intersectionality’, ‘power’, ‘#MeToo/UsToo’, ‘equality’). Figure 2 provides more detail on the proportion of conference items scanned which contained selected terms.

{kind=link}
{kind=link}
Line graph showing % of overall conference content containing specific equity, diversity and inclusion (EDI) terminology.
The presence of EDI-related terms in conference brochures followed a similar pattern where there was a steep increase in 2019 followed by a decrease in 2020, which did not dip below levels observed prior to 2019. For example, the proportion of all keynotes, plenaries and workshops that contained the word ‘diversity’ in their title or session descriptor increased from 0.6% in 2018 to 11.2% in 2019, before dropping to 6% in 2020. An exception to this was the word ‘equity’ where there was a steady increase in the presence of this term from 2018 (0.9%) to 2020 (8%). Also of note was the introduction of new terms such as ‘#MeToo’ which were introduced in 2019, indicating that ongoing discussions related to current social movements were reflected within the programming of conferences.
Discussion
Our environmental scan indicates a dearth of nuanced EDI physician leadership programming and evaluations (question #1). While there were examples of single modules and workshops on structural inequity in the module descriptions, the depth and breadth of EDI content in general leadership programming was lacking. Programmes specific to women (n=6) or UIM physicians (n=2) had more content on issues relevant to these groups. There was limited exploration of intersecting identities and their relationship to structural barriers to academic leadership.
The lack of EDI curriculum in physician leadership programming was mirrored in our search of the peer-reviewed literature for studies of physician leadership programmes that contained a programme evaluation (question #2). While these studies noted encouraging self-reported data, few provided longitudinal analysis or linked self-report data to observable outcomes (eg, promotion and retention rates).
Our scan of conferences yielded different results (question #3). The findings suggest a potential shift in the conversation around EDI in the medical community: there was a noticeable increase in the amount of EDI content at conferences relative to previous years in 2019 where 17% of all keynotes, plenaries and workshops contained EDI content compared with only 4% in 2018. There was also an increase in language related to EDI in conference item titles and descriptors, including terms which are reflective of ongoing social justice movements that centre on challenging structural inequity. Comparing our findings from the peer-reviewed and grey literature on physician programmes with the conferences, it would appear that there may be a growing gap between how EDI is discussed and presented within the medical community and how these concepts are enacted in practice. This gap in knowledge to practice is not unusual, but it underscores a need to continue working toward closing it.
Evaluating whether physician leadership programmes are effective in increasing diversity in physician leadership requires better ways to determine whether programmes are reducing inequities in leadership. There are practical limitations of real-world application at the larger system level. For example, an assessment of even a small number of intersectional categories using traditional quantitative methods may yield findings that are ‘problematic’ because the resulting estimates are statistically unstable or because the small sample sizes make the results unreportable due to local privacy restrictions. Even where they are not problematic, having a large number of results presents significant challenges for developing system-wide policy. Acknowledging measurement limitations, recommending caution in using the results for real-world application, and accompanying changes with planned, integrated evaluations of their impact on all groups of interest should be considered.
A way forward
We have known for decades that structural inequalities are keeping women and UIM physicians out of leadership positions.7 112 To prepare physicians to be advocates of systems change, scholars are focusing on structural competency.113 This approach moves beyond identifying cultural expressions of health and illness (ie, cultural competency) to address how institutional structures and social conditions produce inequalities. According to Metzl and Hansen,113 ‘structural competency seeks to promote skills, not so much for replacing awareness of ‘culture’ in medical settings, but for recognizing how ‘culture’ and ‘structure’ are mutually co-implicated in producing stigma and inequality’ (p128). Leadership training that examines structural inequalities built into medical systems will help physicians understand how complex structures produce inequalities and create barriers to diversity in medical leadership. When physician leaders are equipped with structural competency and agency, they can act in creative ways to transform medicine. There have been further calls from education scholars to not only equip leaders with the means to transform the system, but to call on all involved to consciously act to dismantle the systems that lead to inequity.114
None of the studies in our scan mentioned a theoretical framework related to inequity in leadership using gender/race or other critical social theories. Aligning the purpose of physician leadership programmes with the desired outcome will be essential for these programmes to meet their intended outcomes of creating competent physician leaders who will not just reproduce the status-quo but transforms the structures of medicine. Education scholars have looked at various paradigms of education as a way of understanding the purpose of education, the meaning of learning and the roles that teachers and students play in the process of learning.115 Transformative learning theory is one paradigm for developing leadership programmes that inspire physicians to become agents of change. It involves becoming aware of one’s own and others’ assumptions and expectations, assessing their relevance and forming an interpretation.116 By engaging in critical reflection and discourse, learners develop new ways of perceiving, thinking, deciding, feeling and acting on their experiences.117
Teaching structural competency is challenging, particularly in North America, where most white people lack the awareness of the interactions between privilege and oppression that they need to confront their biases and prejudices.114 For example, in a survey of white medical students and residents, half of respondents endorsed at least one myth about physiological differences between black people and white people, and one third believed that black skin is thicker than white skin.118 We see similar biases in the realm of leadership. In an exercise that asked health professionals at a leadership workshop to envision a leader, none described leaders who were female, racially or culturally diverse, or represented people with disabilities.6 Confronting people with their privilege can provoke responses that range from guilt and shame to anger and despair. Physician leadership training can use the principles of transformative learning theory to identify alternative perspectives, provide emotional support during the process of transformation and help people analyse their interpretations of a situation from multiple points of view to come away with a new perspective.117
Study limitations
Our environmental scan has several limitations. First, searching the grey literature is not straightforward. Using university ratings and limiting the scope to North America to identify physician leadership programmes may introduce bias by favouring long-established and well-endowed institutions. Although there are other ways to identify universities known for world-class research, academic excellence and innovation, the approach we used may have made it easier for other studies to replicate our search strategy. Another limitation of our scan is that it may have overlooked other relevant physician leadership programmes. The programmes in our scan should be viewed as a snapshot of physician leadership programmes with EDI content.
For the peer-reviewed literature, our search was limited to studies published in English. Additionally, only SS reviewed all of the study titles and abstracts to determine which ones met criteria for full text review, which increased the possibility that some studies were missed.
Our scan of medical education conferences also faced challenges. The amount and quality of conference information that we could access varied. Since we could only include conference material that was available to us, we may have missed material that had EDI content. In addition, not including oral conference presentations, which arguably make up the bulk of conference presentations, means that it is likely that we missed material that had EDI content.
Further, we recognise that our construction of diversity also remains limited within the scope of this study. Our own training and identities limit our own perspectives within the very structures we are describing here. We also do not tackle indigeneity, religion, ability, ageism, socioeconomic status differences or other markers that are influenced by structures in medicine and affect leadership in these spaces.
Conclusion
A fundamental question underlies current efforts to increase diversity in physician leadership: how can physician leadership programmes be part of the solution to the identified problem of a lack of diversity? Our environmental scan offers a snapshot that identifies that up to July 2020, most programming still focused on adapting to male white cis-gendered structures. The systematic and ongoing under-representation of women and UIM physicians (among others) requires knowledge of structural competencies to achieve transformational change. The curricula in most leadership programmes seem to focus on individual attitudes without the necessary connection of personal agency to the broader social system. This identified gap between the individual and society will continue to get in the way of increasing diversity in physician leadership if it remains in its current bridgeless state.
We posit that structural competency training in physician leadership programmes provides a necessary framework for implementing curricular reformulation. Physician leadership programmes need curricula that move beyond detailing structural racism and sexism as explanatory factors for a lack of diversity in physician leadership to identifying and addressing the structural factors for these disparities. We also suggest that curriculum developers consider incorporating transformative learning theory, with its emphasis on the social dimension of learning, to bridge individuals’ perspectives and analysis of EDI to the larger social system through strategies such as critical reflection and disorienting dilemmas to become transformative physician leaders in medicine.
Data availability statement
Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We would like to acknowledge Hema Zbogar for her editorial support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ssoklaridis, @Morag_Paton
Contributors SS conceived of the project, the design and implementation of the research, the analysis of the results and the writing of the manuscript. EL contributed to the implementation of the research, the analysis of the results and the writing of the manuscript. GB contributed to the analysis of the results and the writing of the manuscript. MP contributed to the design of the research, the analysis of the results and the writing of the manuscript. CL contributed to the design of the research, the analysis of the results and the writing of the manuscript. RB contributed to the methodology, search strategy and revising of the manuscript. AM contributed to the analysis of the results and the writing of the manuscript. IS contributed to the design of the research and the writing of the manuscript. CRW contributed to the implementation of the research, the analysis of the results and the writing of the manuscript. AK the design and implementation of the research, the analysis of the results and the writing of the manuscript.
Funding This environmental scan was funding by the Society for Academic Continuing Medical Education (SACME) Manning Grant Seed Funding.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.