Article Text

Abstract
Background The academic literature demonstrates that organisational culture contributes to variation between healthcare organisations in outcomes and performance, patient satisfaction, innovation, healthcare quality and safety and employee job satisfaction.
Objectives/methods The aims of this research were: (1) to review literature on organisational culture; (2) to identify the dominant culture within the Belfast RVH Emergency Department by using a combination of both the ‘Organisational Culture Assessment Instrument’ and ‘Rich Pictures’ soft systems methodology; and (3) to formulate recommendations.
Results/conclusion We found that the dominant organisational culture is a market culture (29.74 points), followed by hierarchy culture (28.97 points) then a clan culture (25.55 points) and an adhocracy culture (15.74 points), this infers an emphasis is placed predominantly on results and profitability. The results also look at the difference between current and preferred organisational culture. The largest desired difference can be seen in clan culture, with an increase of 12.93 points. Market culture decreases by 12.39 points. Hierarchy culture decreases with 3.58 points and adhocracy culture increases with 3.04 points. The dominant culture in the preferred situation becomes clan culture, followed by hierarchy culture, adhocracy culture and market culture. The results also show there was a differing gap within all professional groupings with admin (24.97 points), doctors (33.71 points), nurses (40.36 points) and others (11.08 points). The Rich Pictures results highlight contrasting multidisciplinary dynamics in regard to hierarchy, interteam cooperation and a team while working under extreme pressure, and were committed to quality, patient safety and service innovation.
- clinical leadership
- continuous improvement
- engagement
- learning organisation
- values
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Hospitals are human institutions, not buildings, bottom lines, strategic analyses, or five year plans. A hospital is a living organisation—people make a hospital work and its culture ties people together, giving meaning and purpose to their day-to-day activities and lives. (Arnold et al)1
In the end, culture will trump rules, standards and control strategies every single time, and achieving a vastly safer NHS will depend far more on major cultural change than on a new regulatory regime. (Berwick and Shojania)2
The motivation for this research was to diagnose organisational culture within a National Health Service Emergency Department (NHS ED) in Northern Ireland to ensure that positive aspects of the culture are retained and protected, while other cultural features are modified to promote service improvement, collective leadership, satisfaction and reduce physician burn-out.3–5
Belfast Health and Social Care Trust (BHSCT) is one of the largest integrated health and social care NHS Trusts in the UK. BHSCT delivers integrated health and social care to approximately 340 000 citizens in Belfast and provides the majority of regional specialist services to all of Northern Ireland. BHSCT’s annual budget is £1.3 billion with a workforce of over 22 000 (full-time and part-time). This research sampled the RVH Adult ED at the Royal Victoria Hospital with approximately 250 staff. The RVH ED has been under intense pressure and public scrutiny due to patient overcrowding and lengthy patient waiting times. In spite of a toxic environment over the last 4 years, this NHS ED has made significant improvements to quality, patient safety and service innovation.
Qualitative review methodology
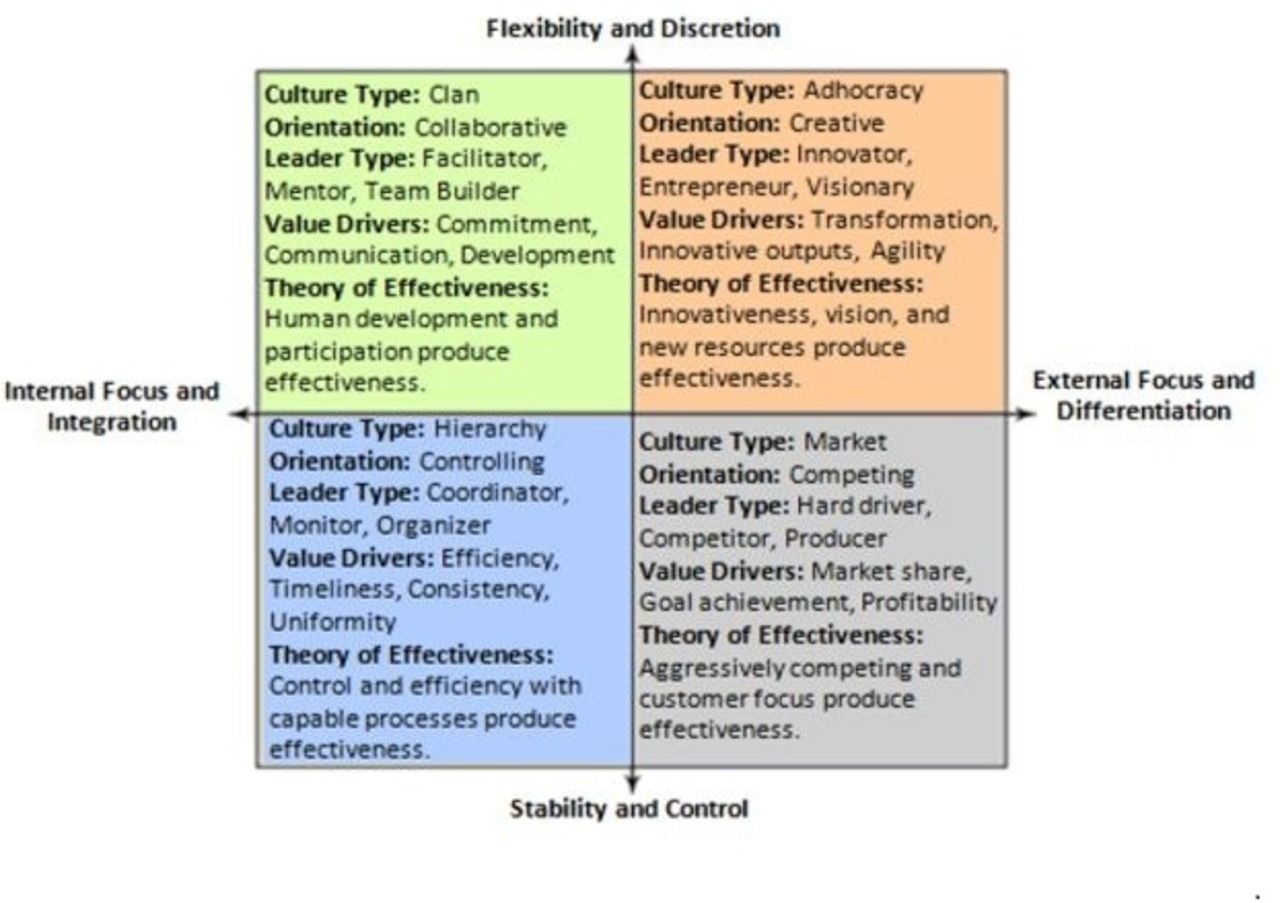
The three aims of this research were: (1) to review literature on organisational culture within the NHS and to identify key themes relating to cultural change, service improvement and collective leadership; (2) to identify the dominant culture within the NHS ED by using a combination of both the ‘Organisational Culture Assessment Instrument’ (OCAI)6 (see figure 1) and ‘Rich Pictures’ soft systems methodology7 (see figure 2); and (3) to formulate recommendations and an implementation plan.
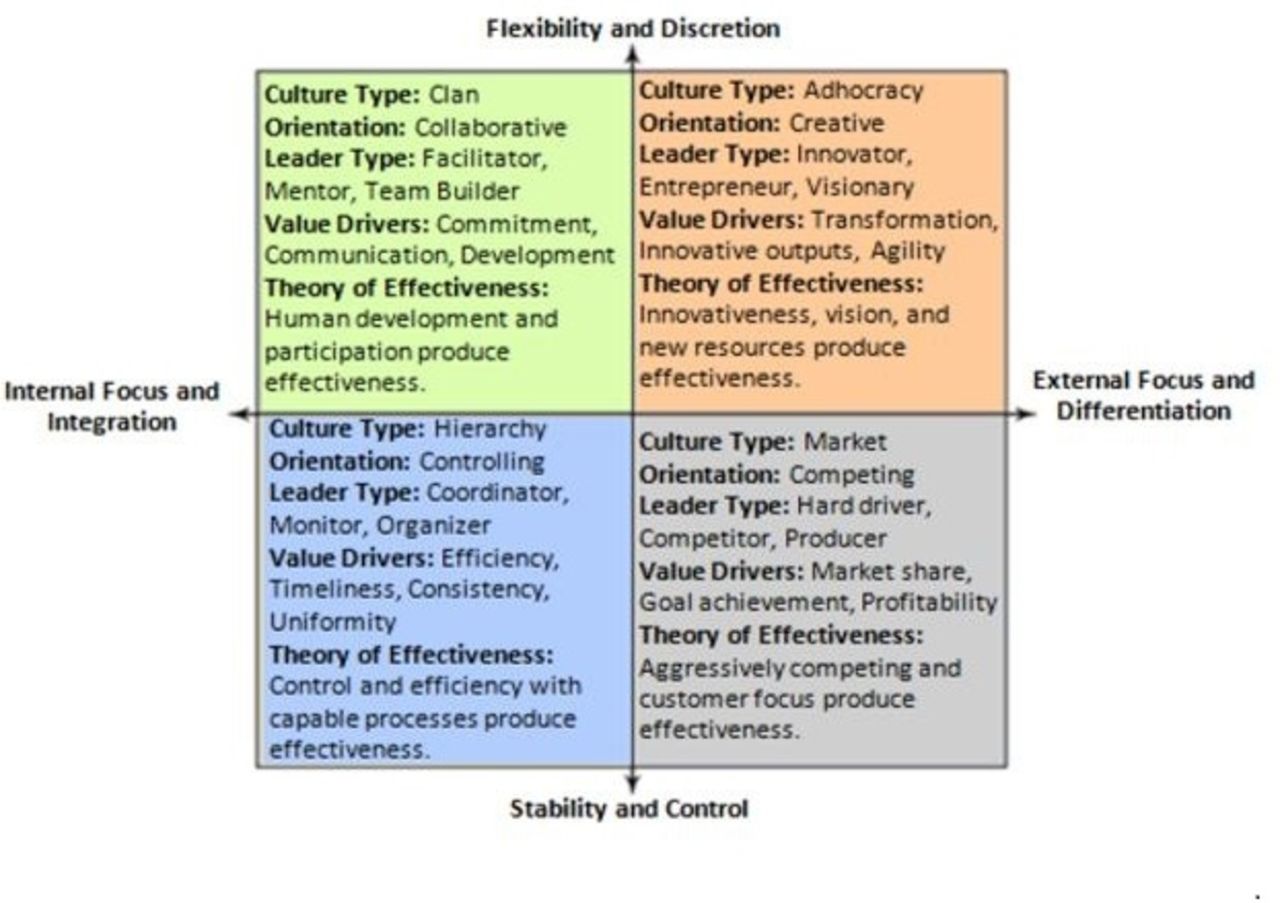
The competing values framework (adapted from Cameron and Quinn [6]).

Rich Pictures (soft systems) methodology.8
By using Rich Pictures the research attempted to draw out the group conversations, emotions, common beliefs, interactions and relationships of key internal stakeholders, to unearth some of their unconscious thoughts and assumptions in regard to perceived organisational culture.8
Findings
The literature review suggests that NHS leaders drive the values of an organisation and those values drive the behaviours. Behaviours collectively become the culture, which in turn drives organisational performance and continuous quality improvement.9 Understanding organisational culture is important because it can be managed. The literature review indicate successful organisations have happier, more productive and engaged employees.10 Successful organisations, with strong culture of creativity and innovation, also encourage employee diversity at all levels through to the boardroom.11 Successful organisations have highly selective recruitment processes ensuring only staff with the right set of values and behaviours are recruited.12
The OCAI survey had a 33% response rate with 83 completed surveys received from the 251 RVH Adult ED staff distributed on 1–23 April 2018. Professional staff participants included: doctors (27 out of 54), nurses (32 out of 144), admin (15 out of 32) and others (9 out of 21).
The OCAI results (see figure 3) indicate the dominant organisational culture as market culture (29.74 points), hierarchy culture (28.97 points), clan culture (25.55 points) and adhocracy culture (15.74 points). There is a mixture of cultures where an emphasis is placed predominantly on results and profitability. The results also look at the difference between current and preferred organisational culture. The largest desired difference can be seen in clan culture, with an increase of 12.93 points, followed by market culture with a decrease of 12.39 points. Hierarchy culture decreases with 3.58 points and adhocracy culture increases with 3.04 points. The dominant culture in the preferred situation becomes clan culture, followed by hierarchy culture, adhocracy culture and market culture. The results also show a differing gap within all professional groupings with admin staff (24.97 points), doctors (33.71 points), nurses (40.36 points) and others (11.08 points). The results demonstrated no congruence was found between the six key dimensions of organisational culture:
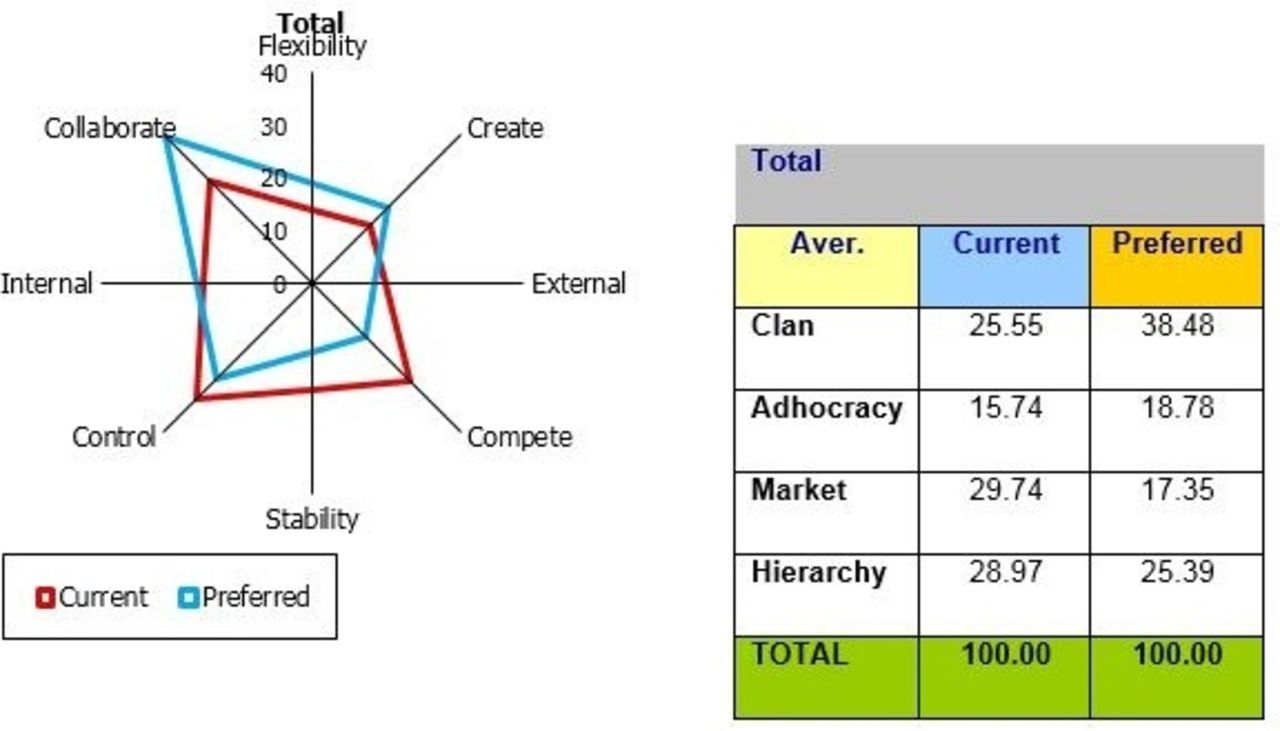
Organisational Culture Assessment Instrument (OCAI) results—RVH Emergency Department.
Dominant characteristics.
Organisational leadership.
Management of employees.
Organisational glue.
Strategic emphases.
Criteria of success.
All professional groups within the RVH ED wish to have more staff empowerment and engagement, greater collaboration and a culture of stronger commitment to the development of people at all levels. In addition, staff wish to see a more creative organisational culture that promotes innovation and entrepreneurship. Staff want no patient overcrowding. Removal of excessive workloads, coupled with less top-down micromanagement and continually changing hierarchical organisational structures and processes are preferred.
The Rich Pictures workshop held on 1 May 2018 had a 12% response rate with 29 participants from within the RVH Adult ED. Professional staff participants included: doctors (4 out of 54), nurses (15 out of 144), admin (8 out of 32) and others (pharmacy staff) (2 out of 21).
The Rich Pictures research results (see figure 4) indicate that staff working within the RVH ED are very proud of their clinical expertise, patient-centred approach and award-winning quality and patient safety multidisciplinary initiatives. However, their working environment is at times very challenging, stressful and target driven, which frequently can leave staff feeling overwhelmed.
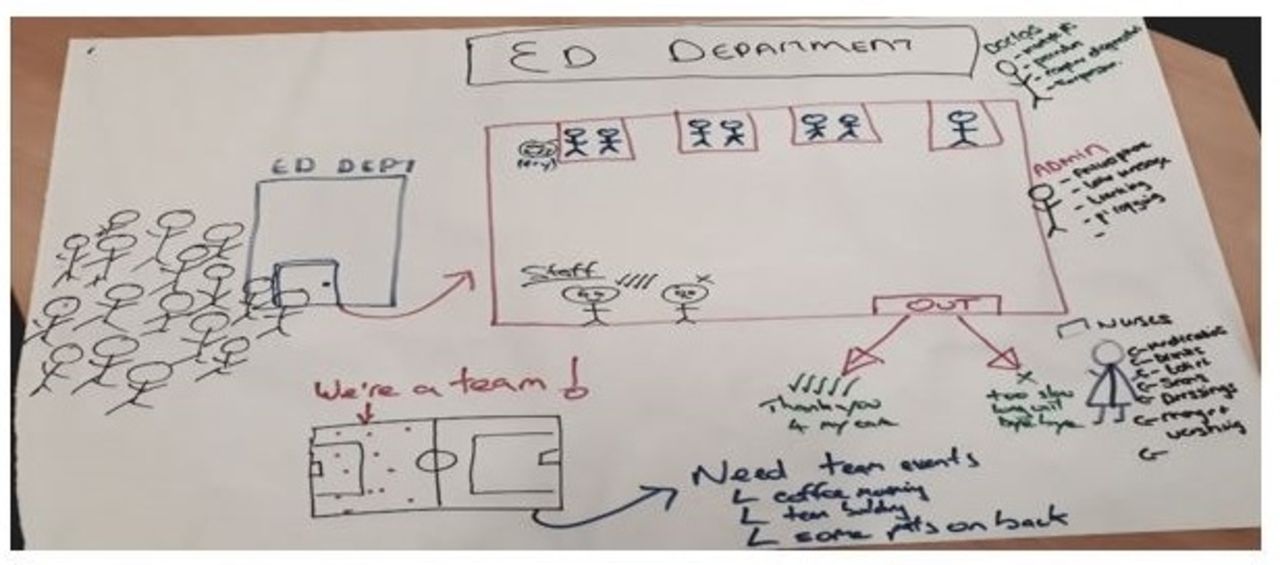
Rich Pictures example picture from RVH Emergency Department.
Staff need support to improve personal resilience and enhance their emotional well-being. NHS needs to provide the time, tools and techniques to augment support for front-line clinical staff. Evidence exists of staff applying quality improvement techniques to everyday problem solving—the result of 90% of front-line RVH ED staff completing online training modules during the last 2 years. Arguably, what is now needed is the cocreation of strategies to improve patient flow and eliminate overcrowding; greater focus on continuous improvement; and an organisation culture where staff feel valued and appreciated. ED staff need more dedicated time to get involved in such quality improvement and innovation activities. Some doctors in Belfast have ring-fenced time within their weekly job plans, however, this is not the case for nursing staff or other professions.
Discussion and conclusion
Summary box
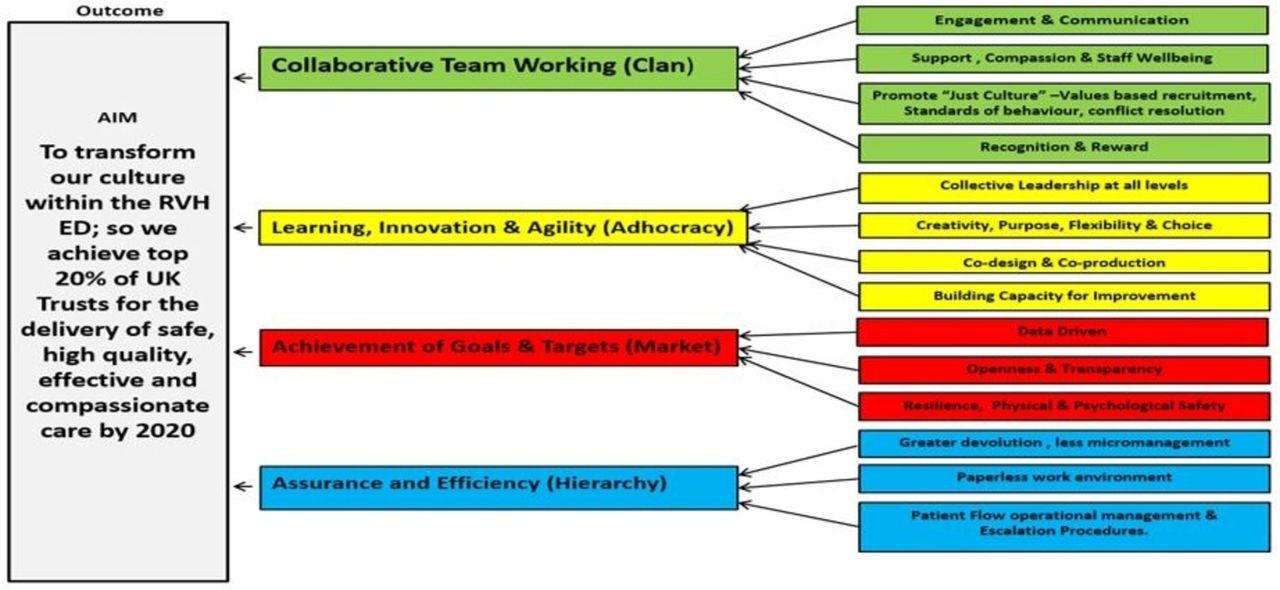
Codesign, coproduction, openness and greater transparency with patients and their families are required. This necessitates greater collaborative working across hospital and community healthcare professions and with the wider regional clinical networks. Collective and collaborative leadership would help remove the current organisational siloes and empower front-line staff. It is anticipated this research will encourage NHS to view their ongoing experience with reshaping their organisational culture from a more evidence-based perspective. It will also help them better understand the deep-rooted embeddedness of current organisational cultural characteristics and behaviours. Finally, it is hoped this research will facilitate greater understanding of the organisation’s culture leading to improved health and well-being of staff and better health outcomes for patients (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Driver diagram—improving organisational culture within an RVH Emergency Department.
Emerging from the research are 10 recommendations to improve organisational culture in a hospital ED. Also mapped are six simple steps to facilitate recommendation implementation. Interestingly, the results of this study, diagnosing organisational culture in an NHS hospital department in Northern Ireland, have greater alignment with public hospitals in China than public and private hospitals in Europe.
Recommendations
The list of 10 recommendations below are designed to assist any NHS ED move its organisational culture towards its desired future state.
Clan culture
Develop and implement programmes to further improve staff engagement and multidisciplinary team building skills within the ED workforce. Consider more frequent and meaningful surveys of employee needs, ideas and suggestions. Ensure staff are comfortable and have the confidence to speak up regarding safety concerns. As part of the roll-out of collective leadership, empower front-line staff by devolving authorisation levels to lower levels and develop ‘cohesive networks’ to help share learning and build new relationships. Energise the staff recognition system within the ED and within the entire NHS, to empower front-line staff and middle-grade managers. Develop a coaching programme for front-line staff and middle-grade managers to help them better understand the strategic pressures and priorities of the NHS, and that outlines how each of their roles must change for the organisation to become more effective and for patient outcomes to improve. Improve cross-functional teamwork by establishing an operational daily ‘safety huddle’ that will provide a plan for that day, identify any immediate organisational risks or concerns and will give a 3-day predictive view into the future. Improve the staff performance evaluation and appraisal systems within the NHS by asking subordinates to assess the performance of their superiors, as well as their own performance.
Continue with organisational ‘value based’ staff recruitment and selection processes. In particular, focus on recruiting staff based on their safety consciousness, team working and behaviours. Work towards a ‘just culture’ which recognises that competent healthcare professions are human and can make mistakes. Identify the specialties or teams inside or outside ED, where there is regular intergroup conflict or disruptive behaviour. Analyse the causes and reasons for such conflict, and design a set of interventions to address outstanding issues.
Adhocracy culture
In a spirit of codesign and coproduction, ensure patients and service users are actively involved in all stages of innovation and service improvement, end to end and top to bottom. Leaders and teams should prioritise quality of care across the system/organisation. Develop opportunities for all front-line staff to receive training in the concepts, practices and responsibilities in regard to a culture of safety, quality and service improvement. Ensure staff from all professions have dedicated time identified to use this training to improve and redesign services. Encourage benchmarking with other organisations both within healthcare and outside to encourage team learning and cross-boundary cooperation, trust and openness. Develop systems, policies and processes to encourage, measure and reward a safety culture and innovation behaviour at all levels of the organisation. Discuss safety culture and opportunities for innovation during leadership walk-rounds, and so on. Critically analyse the current vision statement of the Belfast Trust. Does it provide its key stakeholders, patients and staff with both cognitive and emotional direction? Does it inspire front-line staff to be imaginative and creative?
Roll out and consolidate collective leadership approach to all levels of the organisation, moving away from a highly hierarchical command and control approach to a more flexible and agile-type organisation. Explore the use of new technology and the greater opportunities for digitalisation, in regard to information sharing both within and without the organisation. Establish a repository of links to safety and quality improvement information, resources and best practice. Improve the systems and processes for recording and learning from mistakes, near misses, complaints, clinical incidents and litigation cases. Develop ‘deep dive’ analytics to help triangulate improved learning from these resources. Monitor and evaluate the amount of time executive leaders within the Trust spend on innovation and planning for the future, as opposed to coping with current service pressures, assurance and crisis management. Analyse the organisation’s key values and emphasise in regard to strategic long-term planning, innovation, creativity, service improvement, research and lifelong learning. Encouraging more focus on meeting the challenges of the future. Hold annual ‘innovation’ celebration events at all levels within the organisation and across all directorates, to share safety improvement successes and best practice. These events can also help celebrate new learning (research), and its translation into practice.
Develop a system for r ewarding staff, teams and directorates that recognise creativity and innovation. These reward systems should reward good ideas and assist new ideas being developed and subsequently adopted. Encourage more thoughtfully developed risk-taking and widen organisational diversity to create further opportunities to innovate, by activating the heretics, radicals, disruptors and mavericks within the current workforce, and by balancing the extroverts with introverts within teams. (Too often, there is disconnect within organisations, between the aspiration for radical change and the need to preserve stability and control and the avoidance of risk.)
Market culture
Further improve the current performance management system within the Belfast Trust, by inviting all staff to suggest items that will lead to safer, high-quality and compassionate care, and/or deliver greater value for money. Focus on key goals and adapt to human needs just as much as market needs. Ensure higher level of trust in an employee’s ability to accomplish tasks successfully with less supervision and oversight.
Establish a less of a stressful environment where the drive to achieve productivity and patient waiting time targets do not leave staff exhausted and overburdened. Hold regular focus group interviews with patients and their carers, to obtain better information and feedback on current levels of satisfaction with services. Consider applying the nonadoption, abandonment, scale-up, spread, and sustainability (NASSS) framework for considering influences on the adoption, non-adoption, abandonment, spread, scale-up and sustainability of patient-facing healthcare new technologies,13 while also using parallel annual staff surveys to monitor a subset of organisational culture Key Performance Indicators (KPIs).14 15
Hierarchy culture
Establish new systems for less micromanagement and less rules and process-driven behaviour. Review every corporate policy and procedure, and consider appropriate reductions. Devolve staff recruitment and consumable expenditure approval to line managers nearer the front line, for final sign-off.
Consider using new technology including the adoption of a regional electronic patient record to help move the organisation towards a paperless environment and to help remove unnecessary duplication. Explore the possibility of establishing a more efficient operating system by adopting Toyota’s lean ‘just in time’ practices, to reduce unnecessary waste, harm and variation.
Carry out an assessment of the various significant service disruptions that regularly affect an NHS ED. Develop improved escalation and crisis prevention plans, and crisis response plans, to help improve poor patient flow and patient overcrowding.
Designing and implementing organisational change
The researcher fully acknowledges that implementing organisational cultural change can be very difficult and also can take substantial time. The researcher has synthesised the academic literature and proposes therefore six steps to help improve staff involvement and to minimise resistance from those staff most affected.
Reach consensus of the current organisational culture. This research has shown that both the OCAI and Rich Pictures diagnostic tools are helpful in this regard.
Reach consensus of the desired future organisational culture. Effective staff engagement is crucial at all stages of change to agree buy-in.
Determine what changes are required, and what this will mean for affected staff, and remember the ripple effect.
Identify illustrative stories to help staff understand the journey ahead, and the employer’s expectations.
Develop a strategic action plan. This may include identifying small wins, building coalitions, agreeing accountability arrangements, sharing information, agreeing measurement indicators, explaining why, holding a funeral to celebrate the past and implementing symbolic as well as substantial change.
Develop an implementation plan. Establishing correct leadership style and set of behaviours will be crucial, the literature review carried out for this research indicates that a kind, compassionate, authentic, humble and collaborative leadership style may be most appropriate within a healthcare environment to change organisational culture. The implementation plan will need to cover: required changes in structure, symbols, systems, staff selection and development, strategy, leadership styles and the competence of individuals to carry out the required change processes. Aligning all of these together will be important for successful change.
Acknowledgments
The Belfast Health and Social Care Trust provided support for this research.
Footnotes
Contributors This research was sponsored by the Belfast Health and Social Care Trust. BA designed the study, analysed the data and drafted the manuscript. EF and LS helped distribute survey questionnaires and encourage clinical staff to respond. JM and EG assisted BA to analyse the data, contributed in drafting the manuscript and revising. All authors have approved the final version to be published and are accountable for all aspects of the work.
Funding None required.
Competing interests None declared.
Patient consent for publication Not required
Ethics approval Human Subjects Committee of the University of Ulster (Belfast). The study qualified for exemption.
Provenance and peer review Not commissioned; externally peer reviewed.