Article Text

Abstract
Objectives Medical practice may attract and possibly enhance distinct personality profiles. We set out to describe the personality profiles of surgical and medical specialties focusing on board-certified physicians.
Design Prospective, observational.
Setting Online survey containing the Ten-Item Personality Inventory (TIPI), an internationally validated measure of the Five Factor Model of personality dimensions, distributed to board-certified physicians, residents and medical students in several European countries and Canada. Differences in personality profiles were analysed using multivariate analysis of variance and Canonical Linear Discriminant Analysis on age-standardised and sex-standardised z-scores of the personality traits. Single personality traits were analysed using robust t-tests.
Participants The TIPI was completed by 2345 board-certified physicians, 1453 residents and 1350 medical students, who also provided demographic information.
Results Normal population and board-certified physicians’ personality profiles differed (p<0.001). The latter scored higher on conscientiousness, extraversion and agreeableness, but lower on neuroticism (all p<0.001). There was no difference in openness to experience. Board-certified surgical and medical doctors’ personality profiles were also different (p<0.001). Surgeons scored higher on extraversion (p=0.003) and openness to experience (p=0.002), but lower on neuroticism (p<0.001). There was no difference in agreeableness and conscientiousness. These differences in personality profiles were reproduced at other levels of training, that is, in students and training physicians engaging in surgical versus medical practice.
Conclusion These results indicate the existence of a distinct and consistent average ‘physician personality’. Despite high variability within disciplines, there are moderate but solid and reproducible differences between surgical and medical specialties.
- personality traits
- physician
- difference
- surgeon
- internist
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See:©http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study applied a validated instrument to determine the Five Factor Model personality traits among a multinational sample of >5000 physicians.
The results clearly demonstrate that physicians share a common personality profile that differs from the normal population and is stable across levels of training.
Physicians scored higher in conscientiousness, agreeableness and extraversion but lower on neuroticism.
Between specialties, moderate differences exist: compared with medical doctors, on average, surgeons show lower levels of neuroticism, extraversion and openness to experience.
However, no inferences from the general average personality profiles reported here to the individual physician can be made.
Introduction
A key factor for success in a professional career is how personality traits fit the characteristics of the chosen profession.1 Thus, personality has attracted growing research interest in various professional fields, including medical training, with the aim to improve career counselling, selection processes and training strategies.2
Between different academic fields, personality traits differ.3 Whether or not personality traits of physicians differ from those of the general population remains poorly studied. As only limited data from single institutions are available today,4 5 it is questionable how far the results can be generalised to the entire medical community. But also within the medical field, personality structures appear to differ in students depending on the intended specialty,2 3 6–9 in trainees of different specialties after graduation from medical school,10–14 as well as in board-certified specialists of different disciplines.4 14–21 These conclusions of previous investigations in the medical field remain however limited by somewhat inconsistent results, which were difficult to compare due to small sample sizes and the use of various ways of operationalising and measuring personality traits.
Personality can be comprehensively described using five higher order factors, according to the Five Factor Model (FFM)22 23: agreeableness, conscientiousness, openness to experience, neuroticism and extraversion (figure 1). The present investigation assesses a large, multinational sample of trained or training physicians, using the FFM to describe the profiles of surgical and medical specialties across levels of training.

Personality dimensions of the Five Factor Model and their descriptors according to McCrae and John.30
Methods
Study population and data collection
An online survey was distributed among physicians and medical students in Austria, Belgium, France, Canada, Germany and Switzerland via the management of larger public hospitals offering a variety of ≥10 subspecialisations, official associations of general physicians, official medical journals (Deutsches Ärzteblatt, Germany; Schweizer Ärztezeitung, Switzerland; Le Quotidien du Médecin, France) and students’ councils of the German, Swiss, Austrian and Belgian medical faculties. Data were collected from 12 February 2016 to 12 May 2016. The survey collected the respondent age, sex, primary language, educational level (board-certified physician, resident or medical student) as well as the (intended) medical specialty. A total of 5660 responses were received, of which 512 were incomplete and discarded. Complete answers were provided by 1350 medical students, 1453 residents and 2345 board-certified physicians (table 1).
Demographic data and personality traits of board-certified physicians (specialists), residents and medical students
Measurement of personality traits
All respondents completed the Ten-Item Personality Inventory (TIPI),24 a validated measure of the FFM. This concise instrument employs 10 items to measure the five personality traits, employing a 7-point rating scale ranging from 1 (disagree strongly) to 7 (agree strongly). The set of items is introduced with ‘I see myself as:’, followed by two descriptors per item (eg, ‘extraverted, enthusiastic’; ‘sympathetic, warm’; etc.).23 TIPI was specifically developed for the use in larger samples.24 25 It is available in English, German and French among other languages. Despite less precise estimation of the FFM than with more complex and time-consuming tools, its results have been shown to converge with other widely used FFM measures in self-report, observer report and peer report, test–retest reliability, patterns of predicted external correlates, and convergence between self and observer ratings.24 26 To allow for better comparison, z-scores were calculated, adjusted for age categories and sex using normative population data available for 155 433 women and 122 567 men (Gosling SD, Rentfrow PJ, Potter J. Norms for the Ten Item Personality Inventory, personal communication. 2014).
Hypotheses, statistical analysis and sample size calculation
The first hypothesis was that the personality profiles of physicians differ from those of the normal population. The second hypothesis was that personality profiles of surgeons differ from those of medical doctors. The outcome variables of interest were the age-adjusted and sex-adjusted z-scores of each of the FFM personality traits. The grouping variables were being a physician or not (H1) and being a surgically or medically orientated physician (H2). In line with other research on how personality profiles between two or more groups differ, we assumed that the linear combinations between single personality traits have to be taken into account. Not doing so would imply to discard the multivariate information present in the data. Therefore, we used multivariate analysis of variance (MANOVA) to test H1 and H2. To gauge what personality traits discriminate physicians and normal population (H1) as well as surgeons and medical doctors (H2), we then ran canonical linear discriminant analysis. Post hoc two-sample unpaired t-tests served to illustrate differences in single personality traits between those groups. We further used Bonferroni correction to account for multiple comparisons and Satterthwaite approximation to correct for unequal variances and unequal sample sizes. All statistical tests were two-sided and p values <0.05 were considered statistically significant. Power calculations revealed that to detect a substantially meaningful difference of half a SD between surgeons and internists,4 30 participants per group were required (β=0.9, α=0.001; two-sided). The group sizes present in the sample exceed this number, indicating that the statistical power afforded by the data collected was sufficient to detect meaningful group differences. The software used for statistical analysis was Stata V.14.2 (StataCorp LP, College Station, Texas, USA).
Analysis samples
We restricted our primary analysis sample to board-certified specialists because disciplinary specialisation cannot be considered fixed until board certification. We included students and residents in a secondary analysis sample. Two further amendments were required. To run MANOVA for our first hypothesis, we had to augment our primary analysis sample by a sample of people from the normal population. The authors of TIPI kindly provided means, SD and correlation matrix of all relevant variables for a sample of 305 830 respondents. To test our second hypothesis, that surgeon and medical doctors differ with respect to their personality profiles, we excluded medical specialties as well as diagnostic specialties that did not fit into one of the two categories (online supplementary table 1).
Supplementary file 1
Patient and public involvement
There were neither patients nor the public involved in this research, as the survey was specifically addressed to physicians and medical students. This article will be disseminated to participants of the survey that indicated being interested in the results.
Results
Personality traits of physicians versus normal population
Compared with normative data (n=305 830), board-certified physicians’ personality profile (n=2345) differed significantly, as established by MANOVA (table 2). The subsequent canonical linear discriminant analysis suggested that a main driver of this global difference in personality profiles was the comparably high level of conscientiousness present in our sample of board-certified physicians (table 2). All but one personality trait were significantly different as well, according to unpaired t-tests with Bonferroni correction and Satterthwaite approximation (all p<0.001): physicians scored higher on conscientiousness, agreeableness and extraversion, but lower on neuroticism (table 2 and figure 2). Normal population and board-certified physicians did not differ in openness to experience (table 2). The same analyses performed on our secondary analysis sample, including residents and medical students, replicated the findings with respect to personality profiles across board-certified specialists, residents and medical students (all p<0.001).

Mean z-scores and 95% CIs for each of the Five Factor Model personality traits in board-certified physicians. Y-axis: z-score; X-axis: personality item. A z-score of 0 corresponds to the population mean for the corresponding personality trait in the normative data. All reported p values are from post hoc two-sample unpaired t-tests with Bonferroni correction to account for multiple comparisons and Satterthwaite approximation to correct for unequal variances and unequal sample sizes.
Differences in personality profiles (ie, the individual combination of single personality traits) and personality traits between (1) physicians and normal population and (2) surgeons and medical doctors
Personality traits of surgeons versus medical doctors
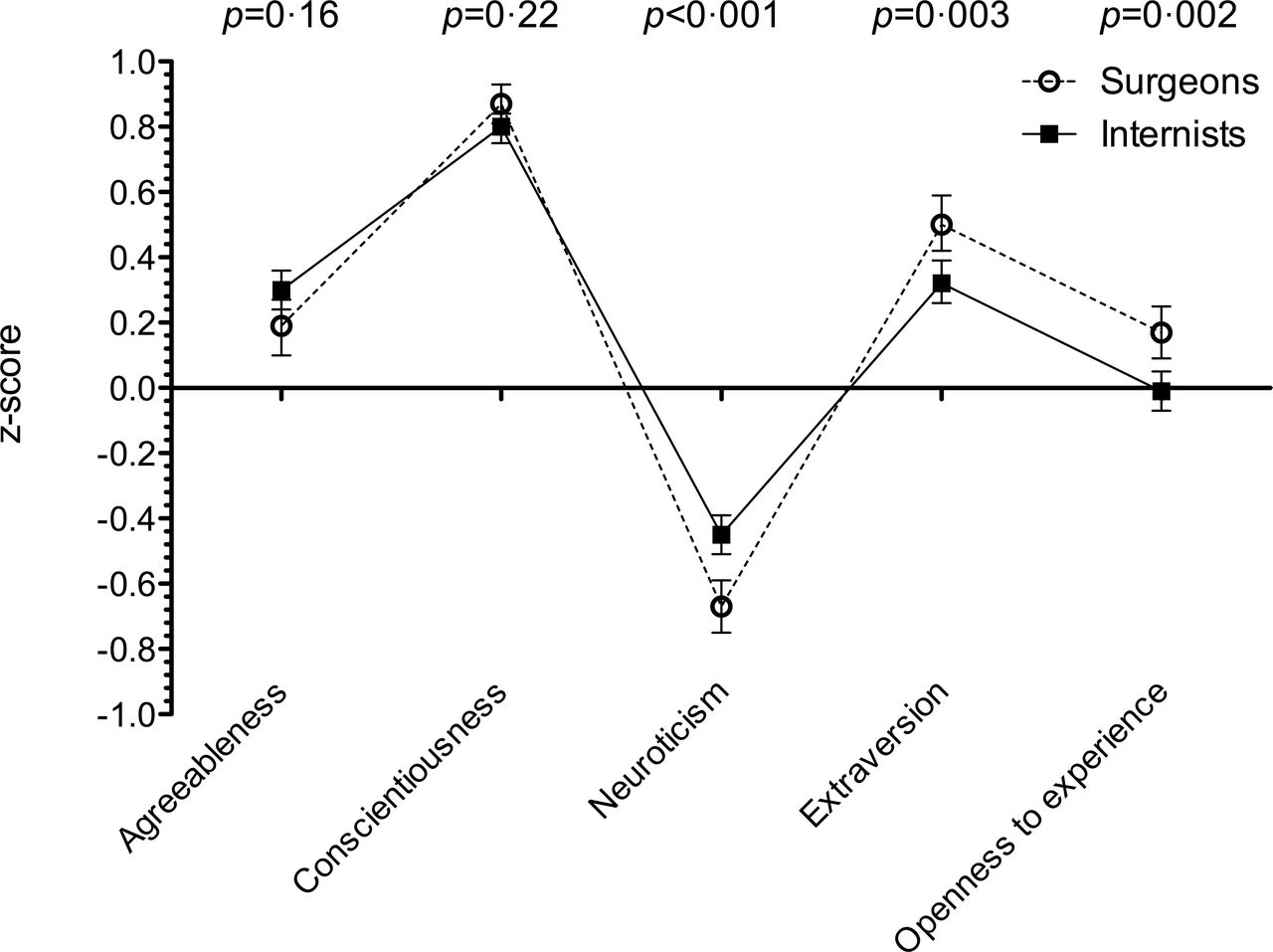
Personality profiles of board-certified surgical doctors (n=465) and medical doctors (n=825) differed significantly (table 2). Canonical linear discriminant analysis revealed that differences in neuroticism mainly drive the global difference in personality profiles (table 2). Turning to single personality traits and using robust t-tests as above, board-certified surgeons’ mean z-scores compared with medical doctors’ were significantly lower for neuroticism, but significantly higher for openness to experience and extraversion (table 2). However, differences in agreeableness and conscientiousness were not significant using a conservative correction for multiple comparisons (table 2 and figure 3). The differences in personality profiles between surgical and medical doctors replicate fully in surgically and medically orientated residents and students.

{kind=link}
{kind=link}
{kind=link}
Mean z-scores and 95% CIs for each of the Five Factor Model personality traits in board-certified surgeons or medical doctors. Y-axis: z-score; X-axis: personality item. A z-score of 0 corresponds to the population mean for the corresponding personality trait in the normative data. All reported p values are from post hoc two-sample unpaired t-tests with Bonferroni correction to account for multiple comparisons and Satterthwaite approximation to correct for unequal variances and unequal sample sizes.
Discussion
The results of this FFM-based personality self-evaluation by more than 5000 trained and training physicians using a web-based questionnaire (figure 1) indicate that physicians share a common personality profile. It is distinct from that of the normal population and stable across levels of training (figure 2). Physicians score higher in conscientiousness, agreeableness and extraversion but lower on neuroticism. The difference in personality profiles is mainly driven by conscientiousness. Between specialties, moderate differences exist: compared with medical doctors, on average, surgeons show lower levels of neuroticism, extraversion and openness to experience, while there is no significant difference in agreeableness and conscientiousness (figure 3). These differences replicate across residents as well as medical students.
Conscientiousness
This trait was previously found to be a significant predictor of success in different professional and academic settings27 28 including medical training.6 12 Qualities associated with the trait conscientiousness, such as efficiency, reliability, responsibility and thoroughness, respond to requirements of medical practice. Low levels of conscientiousness, which may lead to disastrous consequences in some settings, have even been proposed as potential exclusion criterion in the assessment process of applicants to medical school.2 The recent finding that conscientiousness positively predicted the choice of a surgical specialty in medical students9 cannot, however, be explicitly supported by our data.
Neuroticism
Although generally low in medical practitioners, surgeons’ scores were particularly low, at 0.7 SD below the population norm, and a quarter SD lower than in internists (figure 3). Emotional stability can be seen as adaptive to the challenges of medical decision-making, particularly surgical indications and operative practice. Previous studies had already indicated at least equal,10 18 sometimes lower scores29 in surgeons compared with other disciplines.
Agreeableness
As previously shown,4 this trait is prevalent in all physicians. Previous studies reported lower agreeableness in surgeons than internists,9 10 reflecting a generally perceived difference between the two disciplines.4 In the present cohort, differences in agreeableness were not significant among board-certified surgical and medical physicians.
Extraversion
Extraversion is above normal (figure 2) in physicians and more significantly so in surgical than medical specialties (figure 3). This is in line with the majority of previous studies.4 8 18 19 29 Agreeableness and extraversion are the only traits within the FFM directly related to interpersonal interactions. The prevalence of these traits in the medical population intuitively appears appropriate for the physician–patient relationship and also for functional interdisciplinary teamwork.
Openness to experience
There were only slight non-significant deviations from the population norm, positive for surgeons and negative for medical doctors. However, the difference between the two types of discipline is approximately in line with empirical experience and previous data (figure 3).10 18
These findings indicate that, although differences between medical specialties exist, average personality traits are shared between surgeons and medical doctors, as well as students aiming for these specialisations. This large sample therefore highlights with robust estimates that a ‘physician personality’ predominates over ‘specialty-specific personalities’. Although the present data are limited due to its cross-sectional character, the results were stable across the three analysed levels of training.
Since personality profiles predispose towards consistent patterns of behaviour, the consideration of relevant personality traits could facilitate career counselling or even selection processes of applicants to medical school beyond purely intellectual qualifications.2 In addition, in established medical practitioners, a better understanding of predominant personality traits within different disciplines could be helpful for interdisciplinary teamwork and patient care by stimulating self-reflection and professional development.
This is by far the largest study applying a validated measure of the FFM to a multinational and multicultural sample of physicians. The assessment tool (TIPI) is the only existing sufficiently concise instrument to realistically obtain a sample as large as the present one.24 25 Potential biases in the interpretation of the results include age and sex differences, for example, male–female proportions at different levels of training. In the comparative analysis of surgical and medical specialties, these biases were accounted for by adjusted z-scores. Primary language was unbalanced and could theoretically bias the results through differences of mentality and practice patterns. No specific norms for each of the three language areas exist, however. Furthermore, the possibility of producing an intentional favourable image on personality testing should always be borne in mind when interpreting this kind of study. However, social desirability response bias may not substantially distort the results when the questionnaires are administered under ‘non-penalising’ circumstances.2 Another limitation pertains to the comparison of our sample with the norm population data sample, which comprises 60 times as many cases. To assess this potential source of bias, we repeated the analyses on 1000 size-matched random subsamples. These analyses did not lead to substantially different results.
One critical aspect of the interpretation is the assignment of various specialties to the ‘surgical’ and ‘medical’ fields. When the analyses of our study including various specialties, resulting in larger groups, were repeated on very strictly selected but small samples of unequivocal surgical and medical specialties (online supplementary table 2), the findings were reproduced despite the concurrent loss of power. This corroborates the reported findings in the larger groups. Given the scope of this study, it was not possible to draw a random sample from the population of all board-certified and training physicians as well as medical students. Hence, selection bias might limit the generalisability of our findings to, for example, the full population of surgical and medical specialties. Furthermore, it goes without saying that no inferences from the general average personality profiles reported in the present study to individual physicians can be made.
Conclusion
This study suggests the existence of a distinct ‘physician personality profile’. In addition, despite high variability within disciplines, our findings provide evidence for moderate but robust differences in personality profiles between surgical and medical specialties.
References
Footnotes
MNS and FS contributed equally.
Contributors Those persons listed as authors on the manuscript have made substantial contributions to the conception or design of the work, and have been involved in acquiring, analysing or interpreting the data for the work. They all have been active in drafting or revising the manuscript for important intellectual content, which is the basis of the current article. All authors have approved the final version to be published. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Concept: MNS, FS, WS. Data collection: MNS, FS, AW, WS. Data analysis: MNS, RS, FS, WS. Article drafting: MNS, FS, RS, WS. Critical revision: all authors.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was submitted to the institutional review board of the Canton St. Gallen, Switzerland (EKSG 16/020) and the ‘Comité d’Éthique Hospitalo-Facultaire Universitaire de Liège’ (2016/74). Both estimated that it did not fall under the legislation for research involving human beings and that the collected anonymous data did not require any consent beyond the deliberate participation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Once the study results have been published, the data set will be distributed to other researchers upon request. Final decision is made by the corresponding author (MNS) and the last author (WS).