Article Text

Abstract
Introduction The UK is short of doctors, whose workloads have increased. The new role of Doctors’ Assistant has been evaluated with the aim of addressing workload and patient-flow issues.
Methods Five Doctors’ Assistants were introduced at two busy acute hospitals, recruited from the healthcare assistant workforce. We devised a 2-week induction, ongoing supervision and communication exercise. The evaluation used a mixed-method design. Doctors and Doctors’ Assistants completed self-reported diary entries and timings of tasks and ward rounds. Qualitative feedback was sought from other hospital staff and analysed by theme.
Results Diary cards showed 44% of doctors’ time spent on administrative tasks. Doctors’ Assistants’ shifts documented tasks undertaken (including venepuncture, updating patient lists and drafting discharge summaries) with 84% resulting in earlier decision/diagnosis or care. Feedback reported key messages: Doctors’ Assistants provide considerable practical help, their attitude enhances the team and they improve patient flow.
Discussion The project proved safe, successful and well liked. Unexpectedly, the project had to collect financial data to justify its continuation. Acute hospitals have few clinical roles at this level. Role transition requires training, supervision and line management.
Conclusion The role of Doctors’ Assistant should be developed more widely, with attention to detail and economic benefits.
- medical leadership
- doctor
- flow
- health policy
- productivity
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The UK National Health Service (NHS) is short of doctors.1 2 Patients have become more complex with multiple comorbidities, requiring a multitude of interventions. Doctors’ workloads have increased, with burnout and drop-out increasing.3–5
National NHS and educational bodies are training specialist staff to undertake complex aspects of doctors’ work. These initiatives have cost and time implications and some doctors resent them.6 Simple administrative assistance, however, increases physicians’ productivity (patients per hour) by 16% and reduces inpatient stay by 10%,7 with similar results in Southampton8 and Brighton trialling a hybrid administrative and clinical role.
Our setting is an NHS Trust with two busy main acute hospitals, spending over £1 million annually on agency doctor locums at the ward-based level. Our project aimed to test the feasibility of training unregistered staff to undertake a well-defined list of basic clinical and administrative tasks, as delegated by doctors on the wards, freeing up doctors to do more complex tasks or engage in training-relevant activities. We initially aimed to assess safety, training issues, usefulness, acceptability and potential workload. The project changed to assessing financial sustainability.
Methods
Intervention
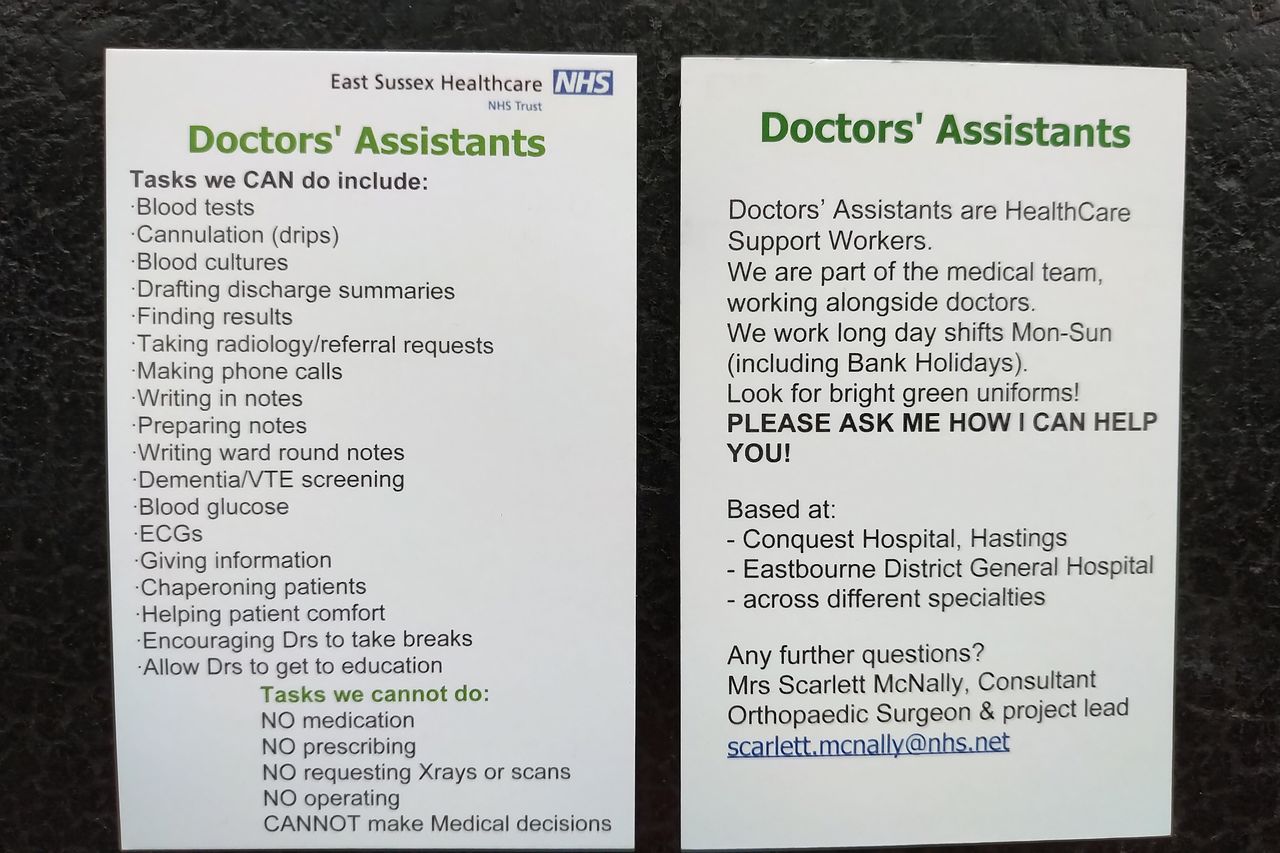
Doctors’ Assistants were introduced in acute medicine at Eastbourne DGH and emergency surgery at Conquest hospital Hastings. They were recruited from within the hospital healthcare assistant (HCA) workforce. We devised a 2-week induction and ongoing supervision plan. Doctors’ Assistants wore bright green uniforms embroidered with their name and role, to help recognition by patients and staff. They were embedded in medical teams with a wide communication exercise, including business cards (figure 1). A grant of £80 000 from Health Education England covered salaries, overtime and on costs for five Doctors’ Assistants for 6 months.
{kind=link}
Photograph of two-sided business card used by the Doctors’ Assistants, detailing tasks. NHS, National Health Service. VTE, Venous ThromboEmbolism.
Evaluation
The evaluation used a mixed-method design, using diary cards and other tools developed in collaboration with University of Brighton. Qualitative feedback, including responses to a semistructured questionnaire, was sought from a range of staff and analysed by theme. Analysis was carried out by SM and confirmed or amended through discussions with JH. Self-reported diary entries were collected. Doctors’ Assistants updated these as tasks occurred verified by patient hospital numbers; doctors completed theirs before the end of their shift. Separately, timings of tasks were undertaken. Variability in emergency workload, shift patterns and doctors’ working styles prevented direct comparisons of doctors’ workload before and after the introduction of Doctors’ Assistants.
As the study progressed, it became clear that financial information was needed for future business case development. We reallocated Doctors’ Assistants to wards to assess their impact on patient flow,9 patient discharge and ward rounds.
Results
Five Doctors’ Assistants completed the 2-week induction and 6-month work secondment after internal recruitment.
Analysis of diary recordings of Doctors
Over 17 shifts without Doctors’ Assistants, doctors’ logs showed 44% of their time on administrative tasks and an average of 70 min overtime per ‘normal shift’. On 28.5% of shifts where an educational session might have been expected, the doctor missed it due to workload. Time studies of doctors’ work showed each discharge summary takes a doctor an average of 19.9 min.
Analysis of diary recordings of Doctors’ Assistants
Analysis of 49 12-hour shifts of Doctors’ Assistants demonstrated considerable variability in numbers of tasks, depending on the day and needs of the team, undertaking: Venepuncture (mean 7.7, range 0–35); drafting Discharge Summaries (mean 4.9, range 0–15); Dementia screening (mean 3.3, range 0–15) and Ward rounds (mean 1.92 hours, range 0.5–3.75 hours).
Financial considerations
This element evaluated ‘patient flow’: speeding diagnosis, care or discharge and freeing beds. In acute medical areas, diary cards from nine shifts showed Doctors’ Assistants tasks could be categorised as: decision/diagnosis earlier 60% (70), care earlier 24% (28), documentation better 4% (5), discharge earlier 3% (4), saving time for doctors 3% (3) and Other 6% (7).
One Doctors’ Assistant attending the elective Orthopaedic ward each afternoon for 12 shifts drafted an average of 5.75 discharge summaries (range 1–12), thus saving doctors around 2 hours’ of administrative work. This is likely to speed up discharges, thus freeing beds and reducing surgical cancellations.
A 4-week trial on the rheumatology/elderly care ward with and without a Doctors’ Assistant identified two instances where patient transport arrived on the ward but was turned away due to discharge summaries not being ready, due to absence of Doctors’ Assistants. The presence of unexpected locum doctors prevented further comparisons.
Ward rounds in Orthogeriatrics and Urology identified useful tasks (eg, finding results, using a laptop, scribing and cannulation). The largest effect on timings was variability between doctors. Attaching a Doctors’ Assistant to a medical post-take ward round (PTWR) identified 27 tasks, of which the Doctors’ Assistant could commence 20; whereas normal practice is for most tasks to wait until the PTWR finishes.
Exception reports detail doctors’ overtime which costs £23 per hour in pay on average with additional fines. Analysis of 232 consecutive exception reports showed 61% (142) reflected a doctor staying late to undertake tasks within Doctors’ Assistants’ capabilities (admin/drips/bloods/drafting discharge summaries).
Qualitative results
Fifty-three individual staff members provided comments. Key messages were: Doctors’ Assistants are considered to provide considerable practical help, their positive approach to work is appreciated and they improve patient flow.
Vignettes were reported and feedback includes: ‘extremely helpful’, ‘Fantastic’, ‘brilliant’ and ‘great’. Doctors’ Assistants also seem to make a difference to how teams work; their positive attitude, reliability and interpersonal skills are praised and many responders express hope that the roles are funded on a long-term basis.
Their effect on the improving patient flow is commended: “The Doctors’ Assistants allow for quicker treatment of unwell patients…eg IV antibiotics”, “They allow for quicker safe patient discharge, improving patient flow”, “[The ward without Doctors’ Assistants] had 13 patients to discharge and one [doctor]—potentially freeable beds in [ward] are blocked for some hours” and “Flow can be translated into beds unblocked and therefore into activity and money”.
Clarifying and introducing the role properly was mentioned and requests for Doctors’ Assistants to be present continuously, over weekends and at specific busy times. The provision of laptops prevents the Doctors’ Assistants from intruding on nurses’ space. Other observations included the need to support the advancement from the original HCA role to Doctors’ Assistant (see box 1). This needs: instant feedback within their medical team, clinical supervision from a senior doctor and good line management.
Items considered essential to the success of the Doctors’ Assistants
Recruitment and training
Previous experience as an healthcare assistant in the Trust, hence both experiential knowledge and awareness of hierarchies and pathways
Induction rooted in values with sessions on behaviours
Training on fundamentals of medical care and prevention (including ‘Making Every Contact Count’)
Regular education sessions, so that challenges are viewed as education not criticism.
Role and team embedding
Doctors’ Assistants embedded in medical teams
Clarity of role and task list
Job plan defined as in band 3 NHS Agenda for Change. This allows them to complete tasks as delegated, but also to prioritise tasks and sometimes to challenge suggested tasks. (Band 5 is for newly qualified, registered staff, including staff nurses.)
Supervision
Awareness that this is a transition from their previous role, which may need careful support.
An educational supervisor who is a doctor (eg, Staff Grade, Specialty Doctor or Associate Specialist (SAS) doctor, registrar or consultant).
A line manager who can manage leave and mandatory employment requirements. This may be an administrator. Their additional workload should be part of the business case.
Communications across all aspects and the wider organisation including patients
Communication exercise across the Trust, so that the role is understood.
Business cards to show skills and the difference from other senior autonomous staff.
Distinctive uniform with role and name clearly visible, for patient and staff recognition.
Thirteen doctors responded to a semistructured email questionnaire. Eighty per cent (8 of 10) who answered the question agreed that doctors would be more likely to attend a teaching session if a Doctors’ Assistant was available to continue delivering clinical work.
Discussion
Our project found 44% of doctors’ time is spent on administrative tasks, including writing discharge summaries, replicating figures of around 50% in other studies.10 Sixty-one per cent of doctors’ overtime ‘exception reports’ resulted from administrative or very basic clinical tasks. This was a real-world study in two hospitals under pressure. Doctors’ Assistants embedded in medical teams allowed direct delegation with feedback; for example, drafting the narrative of discharge summaries could be delegated and separated from doctor-only verifying and adding prescription medication. The biggest differences in timings were variability between doctors. Doctors’ Assistants undertook a variety of tasks in varying numbers depending on service needs, providing flexibility. Feedback was highly positive around practical tasks, attitude and patient flow. Their task flexibility and attitude enhanced team functioning.
Our initial project was to demonstrate need, usefulness, safety, acceptability and concept of Doctors’ Assistants. Unexpectedly, the project had to change to justify the business case for retaining the staff. One Doctors’ Assistant salary is £19 000 pa midpoint of band 3 (2019/2020 figures),11 meaning hospital costs of £25 000 including on costs, overtime, uniform and laptop. The paradox is that vacant doctor posts mean the hospital has no financial outlay if no locum is available. The financial case focused on better patient flow, expediting discharge summaries, reducing cancellation of elective patients and freeing up beds. Eventually, the Doctors’ Assistants were retained as substantive members of staff, with further active recruitment.
The degree to which personal attitude and motivation are praised suggests fortunate recruitment of the right people, but there are limited career opportunities for HCAs in the traditional hospital staff hierarchy. There are very few clinical roles in acute hospitals at band 3 on the Agenda for Change pay scale. Our initial training programme for HCAs to Doctors’ Assistants was successful, with no safety issues. For example, the business cards reiterated that they had no involvement with medication. A whole support structure is required to support individual staff making this transition, with training, supervision and line management. Qualitative feedback from staff highlighted that support and clarity of expectations are key (see box 1).
Concluding messages
Doctors’ Assistants are useful, well liked and safe. Expectations and tasks need clarity. Transition to this role needs good induction, supervision and ongoing support.
Reduction in doctors’ workload is insufficient evidence for acute NHS hospitals to justify new staff salaries. Doctors’ Assistants improve patient flow, facilitating earlier treatment, assessment, investigations and discharge. All these have financial implications for the hospital, which further studies should quantify.
There are no other staff to undertake these tasks and a shortage of doctors. There is clearly a role for delegating basic duties that currently take around half of doctors’ time. The role of Doctors’ Assistant should be developed more widely.
Ethics statements
Ethics approval
Ethical approval was granted through proportionate review (HRA Ref 215636: REC ref17/HRS/0019).
Acknowledgments
Barbara Gosden, Head of Clinical Education who helped plan and run the project. The authors are grateful to the staff at East Sussex Healthcare NHS Trust.
Footnotes
Twitter @scarlettmcnally
Contributors SM led the project, recruitment, training, collecting data. JH helped with design of data collection tools. Analysis was carried out by SM and confirmed or amended through discussions with JH. SM drafted the paper, with JH reviewing and amending the draft.
Funding The project was funded by a £80 000 grant from Health Education England, paying the salaries of the five Doctors’ Assistants for six months.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.